Influence of Vitamin D on COVID-19 (Guidebook) - Benskin
THE INFLUENCE OF VITAMIN D ON COVID-19 OUTCOMES Chapter 4 of Covid-19 and Nutraceuticals: A Guidebook
Bohr Publishers and New Century Health Publishers, LLC
Linda LL Benskin, PhD, RN, SRN (Ghana)
Independent researcher for improving health in rural areas of tropical developing countries, and
Ferris Mfg. Corp., Ft Worth, TX, USA
E-mail: [email protected]
“Light is sweet and it pleases the eyes to see the sun.” — Solomon Hebrew King and Philosopher
ABSTRACT
Most of the world’s population has vitamin D levels which are suboptimal for healthy immune system function. Recent recommended goals are far higher than legacy guidelines, which are based entirely upon promoting bone health, rather than on supporting all the many other functions of vitamin D. Vitamin D strengthens the innate immune response, decreasing the likelihood of infection from SARS-CoV-2 exposure. Vitamin D also regulates the adaptive immune system and inflammation. Thus, with appropriate levels, infected persons have a reduced likelihood of developing hyperinflammatory (severe) Covid-19 (the cytokine or bradykinin “storm”). Many experts have noted that vitamin D plays a role in preventing every one of the disorders associated with severe Covid-19. In addition, the risk factors for getting severe Covid-19 are identical to the risk factors for becoming vitamin D deficient. Evidence of a link between low vitamin D levels and poor Covid-19 outcomes is robust, including numerous population and individual correlational studies, causal modeling, prospective cohort intervention studies, and randomized controlled trials.
📄 Download the PDF from Vitamin D Life
Background
The industrial revolution led physicians such as Sniadecki (in Poland, 1840) to notice that sunlight is protective for human health.1 He noticed that children living in the crowded, polluted city of Warsaw developed rickets, while children living in the nearby countryside remained rickets-free.1 The hypothesis that sunlight on skin could influence the deep tissues and bones was initially met with skepticism, but the evidence became undeniable: in 1900 over 90% of European urban children and 80% in Boston suffered from rickets.1 Though cod-liver oil had been used to treat and prevent rickets for years, in the early 1900s, UV-irradiated fat (“vitamin D”) was identified as another cure.1,2 In 1928, Adolf Windaus was awarded the Nobel Prize for discovering “vitamin D.”2,3 In 1936 it was discovered that UV light from sunshine produced D3 in the skin, which is then converted by the body to biologically active 25(OH)D, which means that “vitamin” D is, in fact, a steroid.2
In 1979, a team led by Stumpf discovered Vitamin D receptors throughout the body, revealing that vitamin D is important for more than just skeletal calcium maintenance.1 Evidence gradually emerged that vitamin D is among the most powerful of the micronutrients, with receptors in virtually every body system.4 Through its local actions (autocrine and paracrine signaling), vitamin D helps regulate processes as varied as insulin production, apoptosis, and innate and adaptive immunity, thus affecting infectious disease vulnerability and most inflammation-related conditions, including hypertension, diabetes, cancer, arthritis, cardiovascular disease, and autoimmune diseases.1,5-7
Prior to the industrial revolution, virtually all of humankind hunted, gathered, farmed, and fished while the days were long, gaining body-weight and storing vitamin D in their fat and muscle tissue.8 When the dark winter came, opportunities to obtain food diminished. As people lost weight, vitamin D was released, promoting continued good health.9 The industrial revolution led to a more indoor, often sedentary lifestyle, and more wealth for the masses, so that people with chronically low vitamin D levels gain weight not only during the harvest, but also throughout the winter, without exerting their muscles as much. Their blood “vitamin D” levels drop precipitously, reaching critically low levels by the time the next summer arrives. For example, vitamin D insufficiency is >85% in the winter and spring among pregnant women in Southern England, dropping to 30% in the summer.10 In Ireland, 24% of the population is vitamin D insufficient (calcifediol <20ng/ml) in summer, more than doubling to 49% in winter 11 Rare optimal calcifediol levels (>40ng/ml) were found primarily in older women (1-7%), who would be most likely to take supplements year-round for bone health.11-13
Because the UVB rays required to produce vitamin D in skin are obstructed by air pollution, clouds, window glass and even ozone when the sun is low (below a 45 degree angle, as is the case in winter, in areas far from the equator, and in the early mornings and late afternoons), and the only significant dietary sources of vitamin D are wild-caught fatty fish (which feed on sunbaked plankton), vitamin D deficiency has traditionally been addressed with food supplementation.1,14,15 However, supplementation (except in Nordic countries) has decreased over the years, consumption of foods traditionally fortified in some countries, such as cow’s milk, is declining, and humans worldwide are adopting an affluent (obese), indoor lifestyle.16 Individuals with naturally melanin-rich skin who live outside the tropics are rarely able to obtain sufficient vitamin D from the sun.17 As a person ages, the ability of their skin to produce cholecalciferol decreases.18 All of these factors led to an alarming vitamin D deficiency pandemic long before Covid-19 appeared on the scene.16,19,20
Covid-19 is caused by a novel coronavirus, but the symptoms of severe Covid-19 are not at all without precedent. Respiratory viral illnesses of the past: the Spanish flu of 1918, SARS, and MERS, are quite similar, and even dengue fever has the same basic history of illness.16,21,22 In each case, the initial viral illness is mild or asymptomatic for most people, with some sufferers developing symptoms more like influenza. However, as they appear to be recovering (and their viral load is dropping), a few people suddenly take a turn for the worse, because their immune system over-reacts.23,24 This immune system overreaction, not the virus itself, causes life- threatening hyper-inflammation.22,23 In the case of Covid-19, macrophages, cytokines, and fibroblasts fill the lungs, which leads to difficulty breathing. , - The increased inflammation can also lead to blood clots and organ damage.23,26 We know the virus itself is not the proximate cause of this organ damage because researchers do not find viable virus in the blood of Covid-19 26 28 29 sufferers, even when they have severe Covid-19. , , The rare exceptions seem to be when the virus is forced into the blood stream from the lungs by high pressure ventilator treatment.
It is well known that vitamin D helps prevent chaotic immune responses such as those characteristic of severe Covid-19 (the cytokine or bradykinin “storm”).30 Therefore, it should be expected that many Covid-19 sufferers will have low levels of vitamin D. Already by March, 2020, dozens of published studies demonstrated that low vitamin D levels lead to poor Covid-19 outcomes.16 As of June 2021, a link between low vitamin D levels and poor Covid-19 outcomes was asserted in ~3000 published studies and biological plausibility discussions in MEDLINE indexed journal articles, including hundreds of population and case correlational studies, causal modeling, RCTs, and prospective cohort intervention studies. At this point, multiple metaanalysis author groups have concluded that there is a significant relationship between 25(OH)D serum levels and Covid-19 infection, severity and/or mortality.4,31,32
Classification of vitamin D levels and why low levels are common
Defining Vitamin D
Confusion about vitamin D complicates the design and obscures the interpretation of research studies.33 Four different molecules are commonly called vitamin D. (See Figure 1, page 4)
Cholecalciferol , or vitamin D3, is produced when UVB light (primarily 295-300nm) acts on 7-dehydrocholesterol in the skin to break the ring between carbon 9 and 10. Wild caught salmon and other fatty fish whose food-chain begins with sun-exposed plankton are rich in D3; far lesser amounts are found in free-range eggs and cheese.30 However, without added UVB skin synthesis or supplements, only an almost exclusively wild fish diet will provide adequate vitamin D. Cholecalciferol is the most common vitamin D supplement, easily extracted from sheep lanolin. Before this process was discovered, Ergocalciferol, or vitamin D2, supplements were common. Ergocalciferol, which is one third as potent as cholecalciferol, is formed in modest amounts when mushrooms or yeast are irradiated with UVB light.34 Fruits and vegetables do not contain significant vitamin D. In some countries, foods are fortified with vitamin D2 or D3, but often at only modest levels. Because cholecalciferol, which stabilizes the endothelium and is in itself anti-inflammatory, and has a half-life of only 24-50 hours, sunshine and/or D3 supplement intake should ~~#00F:ideally be daily, rather than at less frequent intervals.3,6,35
Vitamin D Life disagrees: See Better than Daily ~~
Calcifediol , 25(OH)D, 25hydroxyvitaminD, and calcidiol are all names for the form of vitamin D that is produced when the enzymes CYP2R1, CYP27A1, etc. in the liver replace the H with an OH group at the 25 position of cholecalciferol.36,37 Ergocalciferol is converted to calcifediol as well, but the process is less efficient. Because calcifediol has a half-life of about two weeks, appropriately increased weekly vitamin D intake provides almost as many benefits as daily.38
Calcitriol , also called 1,25OHD or 1,25(OH)2D, is produced when CYP27B1 replaces the H at the 1 position in calcifediol with another OH. This tightly regulated process takes place in the kidneys for circulating calcitriol used in calcium transport, but it also takes place in other organs, monocytes, and macrophages (see diagram).39 The vitamin D receptors found throughout the body are activated only by calcitriol and its analogs.
The ubiquitous enzyme CYP24A1, induced by high calcitriol levels, adds an OH to the 24 position of calcifediol and calcitriol. This irreversible process leads to the formation of calcitroic acid, which aids in callus formation for fracture healing, but appears to be otherwise inactive and is rapidly excreted, protecting against toxic vitamin D levels.37,40 A single bolus dose of cholecalciferol can lead to increased calcitroic acid production for at least 28 days.41
The photochemistry of vitamin D biosynthesis in animal and fungi: UVB light breaks the ring between C 9 & 10
Note: In general, plants do not contain the cholesterol needed to synthesize vitamin D. Vitamin D2 (fungi) is one-third the potency of vitamin D3.
Liver hydroxylation of cholecalciferol (D3) to calcifediol, which is 25(OH)D: H at position 25 is replaced with OH 25(OH)D hydroxylated by the monocytes and macrophages:
25(OH)D hydroxylated by > 36 other tissues , including the prostate gland, breast, placenta, colon, lung, parathyroid gland, keratinocytes, brain, pancreas P cells, cardiac muscle, thymus, and cancer cells: Regulates differentiation and cell growth in those organs, cell signaling.
Kidney hydroxylation of calcifediol to calcitriol, which is 1,25(OH)2D: H at position 1 is replaced by OH
(Calcitriol is also formed, in lesser quantities, in the monocytes & macrophages, and in the many tissues with vitamin D receptors)
Circulating CYP24A1 adds an OH to the 24 position of calcifediol and calcitriol in response to high calcitriol levels to form calcitroic acid, which is excreted, helping protect against toxicity. Calcitroic acid can be mistaken for calcifediol by many tests for 25(OH)D.
Differences in units used to report blood levels of vitamin D and to discuss supplement dosages can also be confusing. Serum 25(OH)D is reported in either ng/ml or nmol/L. To convert ng/ml to nmol/L, multiply by 2.5 (20ng/ml = 50nmol/L). For vitamin D3 taken by mouth, the conversion factor from mcg to IU is 40 (50mcg = 2000 IU).
Although cholecalciferol and calcifediol both circulate in the blood, cholecalciferol is more easily absorbed into muscle and fatty tissue.8,36 Serum vitamin D tests measure total calcifediol, but most are cross-reactive with calcitroic acid that has not yet been excreted, which can mislead researchers. 36 Calcifediol, rather than cholecalciferol, supplements are appropriate for individuals with chronic kidney disease, because their elevated parathyroid levels inhibit the conversion process in the liver.42 Individuals with liver failure may also require calcifediol.36
Recently it has been learned that giving calcifediol rather than cholecalciferol also leads to a much faster and a 3-6 times larger increase in available active vitamin D (calcitriol)42,43 This has significant implications for remedying vitamin D deficiency in acutely ill patients, as it can take up to 7 days for large doses of cholecalciferol to be converted to calcifediol naturally, and a much higher percentage is lost to storage in the fatty tissue.42 However, raising calcifediol levels too rapidly can cause rapid catabolism while dramatically increasing calcium levels.37 As was mentioned earlier, this catabolism may mislead researchers who are unaware of the fact that most 25(OH)D tests do not distinguish between circulating calcifediol and unexcreted calcitroic acid 36. Therefore, extended release calcifediol or multiple moderately high doses should be used.37 Research into the **reasons intensive care patients often require 10 - 100 times the normal dose of cholecalciferol to raise their 25(OH)D levels above 20ng/ml is ongoing_, but it appears related to decreased CYP2R1 activity induced by fasting, diabetes, obesity, exposure to high-dose glucocorticoids, illness, and other factors.39
Recommended serum levels and intake goals from organizations and governments
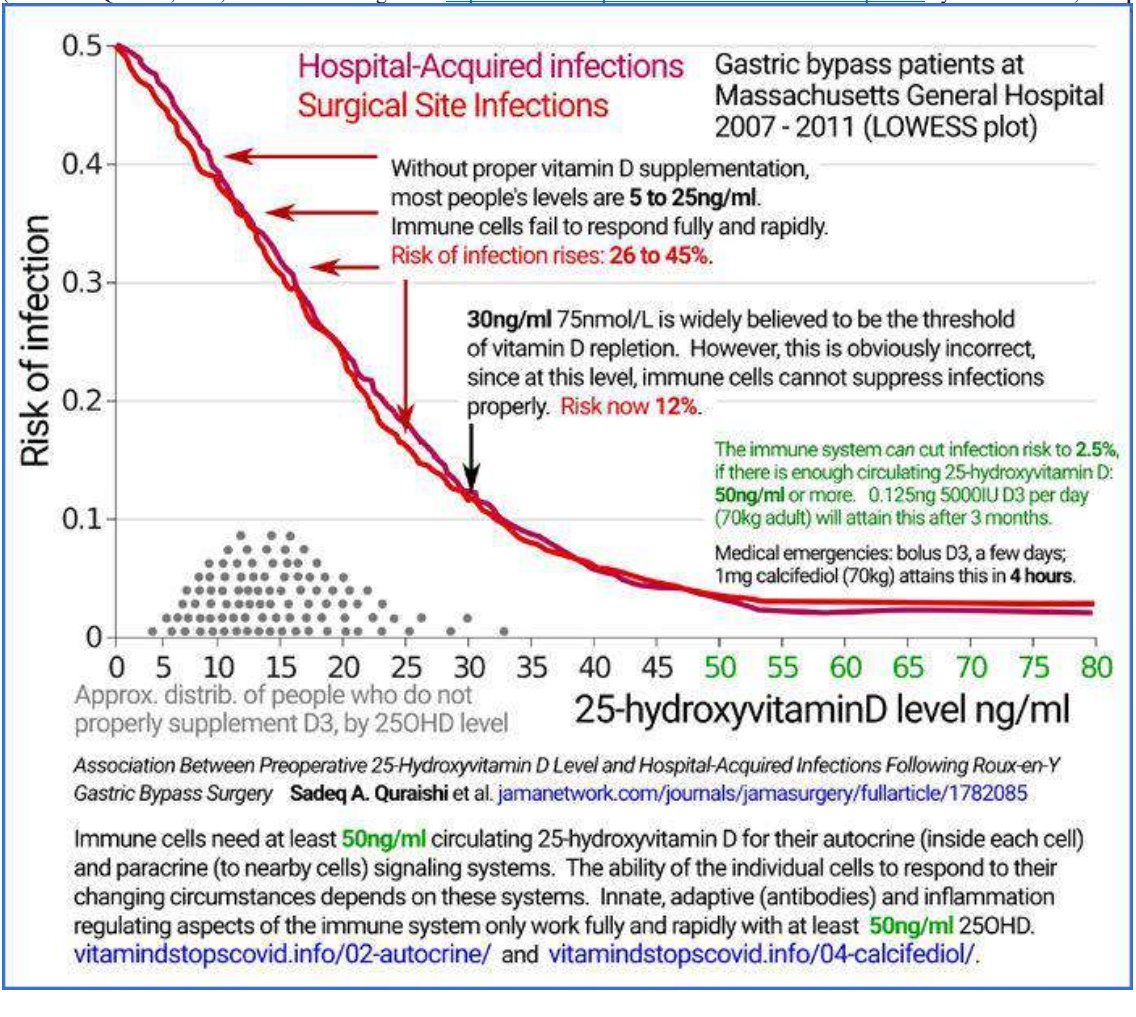
Most legacy public health guidelines for target serum vitamin D levels, based entirely upon supporting bone health, define <10-12ng/ml 25(OH)D as “vitamin D deficient” and <20ng/ml as “vitamin D insufficient.”16 However, clinical practice guidelines that take into account the many other functions of vitamin D widely recognize that levels below 30ng/ml are insufficient.10,37,44 Most researchers define 25(OH)D levels below 20ng/ml as deficient.16,44 Parathyroid levels are elevated for all races, which would logically indicate that a deficiency exists, when 25(OH)D is below 32ng/ml.45-47 When living a traditional lifestyle in the tropics, the Hadzabe and Maasai of East Africa have mean 25(OH)D levels of close to 50ng/ml, as do lifeguards 48,49.* Both surgical and hospital-acquired infection rates plateau at very low levels when 25(OH)D levels reach 50ng/ml. 12 Researchers evaluating 191,779 PCR test results from a laboratory database found that Covid-19 positivity rates also plateau at very low levels when 25(OH)D reach 50ng/ml *.50 (See Figures 2 and 3, page 6)
The National Academy of Medicine, the UK’s NICE and most other public health policy organizations recommend age-dependent daily intakes of vitamin D3 in the range of 100 - 800 IU, with a goal of reaching serum 25(OH)D levels of 20 - 50ng/ml.51,52 However, two groups of researchers have evaluated the data and concluded that the statistical calculations used to determine these recommended intakes contain an error.51,53 A third group agreed, finding that the recommended vitamin D3 intake for adults to reach only the minimal 20ng/ml serum levels needed for bone health could be over 7000 IU/day.54,55 Because circulating levels of 30ng/ml or greater are required for the immune cells to convert calcifediol to calcitriol, 40-60ng/ml is recommended.7,56
The Endocrine Society recommends 2000 IU of vitamin D3 daily for most adult patients to reach their minimum target 25(OH)D level of 30ng/ml, but acknowledges 4000 - 6000 IU/day may be required for obese and malabsorptive patients, and that up to 10,000 IU/day is safe.7,51 Recent research exploring the role of vitamin D in maintaining immune health, regulating inflammation, and helping prevent autoimmune diseases, cancers, allergic disorders, infections, skin diseases, neuropsychiatric disorders, and cardiovascular disease has led to further support for higher supplementation recommendations.57 Serum 25(OH)D levels of* 40-60ng/ml are now considered optimal for immune health , and even higher levels are recommended for treating 12 autoimmune and many other serious health conditions. *7’45’46’58’59 Vitamin D’s critical autocrine signaling requires 25(OH)D concentrations of 40-60ng/ml to function properly.7
Figure 2: Relationship between circulating 25(OH)D level and COVID-19 positivity rate 50
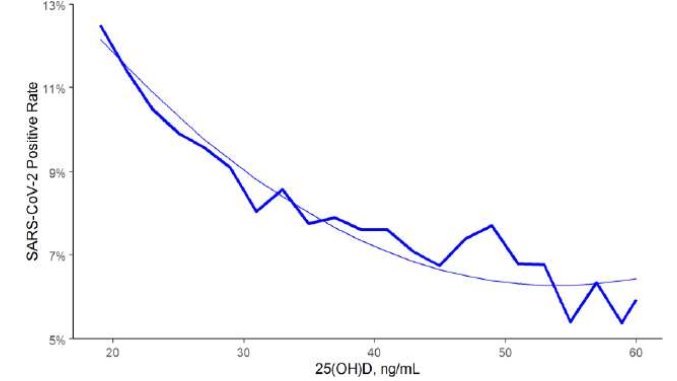
Figure 3: Relationship between circulating 25-hydroxyvitamin D levels and risk of infection12
The vitamin D deficiency pandemic began long before Covid-19 appeared on the scene.16,52,60 In the USA, in Minnesota (44°N), 60% of the immigrant and refugee population suffer from vitamin D insufficiency, as do 40% of all Canadians and 56% in the UK.61 Not surprisingly, the highest risk groups for vitamin D deficiency mirror the those of severe Covid- 19: people who are elderly (particularly those living in care homes), obese, hypertensive, diabetic, male, have naturally melanin-rich skin and live outside the tropics, or those who live in areas with high levels of air pollution.16,17,22,62
Despite this, many public health officials continue to discount vitamin D supplementation during Covid-19, with the WHO recommending 200-600 IU, depending upon age, for individuals who are not able to take in sunlight due to lockdowns, and the NHS and British Dietetic Association continuing to suggest 400 IUs for sun-starved adults.63-65 As of 5 Sept 2021, the US NIH had no official stance on vitamin D for the prevention or treatment of Covid-19, noting that deficiency is the most common in groups that are hardest hit by Covid-19 and biological plausibility is strong, but there is a theoretical risk for toxicity with high doses; the only study cited is one in which the authors of the page themselves note that vitamin D3 was given to patients very late in their illness.62
(Toxicity is very low – much lower than for Vitamin D)
A hypothetical concern for toxicity (serum 25(OH)D>150ng/ml), often mentioned while stating that vitamin D is a fat soluble vitamin (harkening to vitamin A) is the main reason given for not recommending population-wide vitamin D supplements.66 However,* vitamin D toxicity is far more rare than vitamin A toxicity , in part because of the built in fail-safe described earlier.37 What is called vitamin D toxicity is, in fact, calcium toxicity *, and it occurs only in extreme situations: when calcium intake is far too high; when the person has serious calcium-altering diseases (e.g., primary hyperparathyroidism, tuberculosis, lymphoma, sarcoidosis, or other granulomatous disorders); or when the person ingests doses of vitamin D in excess of 20 times the upper recommended dose of 10,000 IU for prolonged periods of time, which has happened historically primarily as a result of errors in manufacturing, labelling, or prescribing.66,67
Even when hypervitaminosis D occurs, treatment is simple and permanent damage is rare.68,69 A large ecological study of high vitamin D supplementation took place by accident when in 1990-1992 a dairy in the Boston area accidentally fortified milk with 230,000 IU/quart instead of 400 IU/quart: 575 times the intended amount.70* The overage remained undiscovered for two years *, as despite taking in this high dose day after day most customers did not become ill; but eventually Boston area emergency departments linked the resultant approximately 19 cases of vitamin D toxicity to the dairy.70,71 The only sufferer who did not recover died of pneumonia due to immune compromise from the prednisone given her as treatment, rather than from effects of hypercalcemia.70,72 The jury found that the dairy’s dramatic error did not cause the decedent’s death.72
Virtually all experts agree that up to 10,000 IU/day of D3 is safe, long-term.66,67,73 Studies of vitamin D supplementation consistently find no differences in adverse events between controls and treatment groups, despite up to 50,000 IU/day being given, long-term. , - Patients receiving short-term high dose (60,000 IU/day) vitamin D3 therapy for Covid-19 raised their 25(OH)D levels to 39-113ng/ml without a significant increase in their calcium levels.77,78
Biological Plausibility: How vitamin D’s known mechanisms of action relate to Covid-19
Multiple vitamin D functions are relevant to Covid-19 outcomes. At the most basic level, vitamin D reinforces natural barriers against respiratory tract invaders, preserving the tight, gap, 52 79 80 and adherin junctions between epithelial cells. , , Vitamin D strengthens the innate immune response, significantly decreasing the likelihood of exposed individuals becoming ill with a respiratory virus at all, with modest daily doses being far superior to larger monthly doses. , , Vitamin D also controls the adaptive immune response, providing a robust response to the viral threat while calming excess inflammation, which should help prevent the acute respiratory distress syndrome (ARDS) that is responsible for ~70% of Covid-19 fatalities. , - Through its regulation of the renin-angiotensin system (RAS), vitamin D directly limits the initial severe Covid-19 complication, ARDS.22 Vitamin D also protects against thrombolytic events, which affect 28% of ICU patients with Covid-19.22,82,84 Therefore, one should expect individuals with higher vitamin D levels to be less likely to test positive for Covid-19, to be hospitalized due to Covid-19, to require ICU or ventilator care, and to die of Covid-19. The evidence, reviewed later in this chapter, supports this expectation.16
Optimal 25(OH)D levels can more than halve the incidence and significantly reduce the duration of acute respiratory infections by enhancing the innate immune response, including increasing vitamin D dependent antimicrobial peptides, such as cathelicidins and defensins.81,85,86 Cathelicidin LL-37 is antiviral, and it also helps regulate inflammation during illness.31,87 Supplementation with 4000 IU/day of vitamin D decreased dengue virus infection.88
The adaptive immune response to SARS-CoV-2 relies upon memory and regulatory T cells, which are heavily dependent upon adequate vitamin D levels.81,89 People who have had asymptomatic or mild Covid-19 have robust memory T cell immunity which persists post infection.90 In contrast, patients who died of severe Covid-19 had impaired T cell responses, which would permit auto-immune responses while allowing the SARS-CoV-2 virus to reproduce unchecked.25,90 Vitamin D regulates the adaptive immune response, recruiting neutrophils, macrophages, and dendritic cells early in the infection while limiting maturation of dendritic cells to prevent excessive inflammation.91 Vitamin D suppresses excess T helper type 2 cell responses and induces T regulatory cells to inhibit inflammation, improving adaptive immune system functioning.57
Vitamin D increases anti-inflammatory cytokines such as IL10 and decreases pro- inflammatory cytokines such as IL1, IL6 and TNFa.16,32,91 Vitamin D deficient Covid-19 patients had significantly higher serum IL-6, TNFa, and ferritin levels than did patients with higher 25(OH)D.92 Prospective trials of high-dose daily vitamin D treatment for Covid-19 have also found significant decreases in inflammatory markers (CRP, IL6, LDH, fibrinogen, and ferritin) when compared with pretreatment levels and controls.77,78 Vitamin D also inhibits MMP-9, bradykinin, and CRP.83,93 Therefore, one would expect vitamin D to help prevent Covid-19’s infamous cytokine or bradykinin “storm”.30,80
ACE2 receptors, to which SARS-CoV-2 binds in the lungs, are highly expressed on surfactant-producing type 2 pneumocytes.83 By disrupting these pneumocytes, the virus decreases surfactant production, causing the alveoli to collapse.83 Calcitriol increases ACE2 expression, which could prevent this complication.83 ACE2 helps protect the lungs against ARDS.32 Vitamin D deficiency, which is more common in older males than females in many areas, is associated with increased X-chromosome-linked RAS activity.22,94 For this reason, males are far more susceptible to ACE2 receptor dysregulation and the resultant hyperinflammation that is the hallmark of severe Covid-19.94 This role of vitamin D alone strongly suggests a protective role against severe Covid-19.22
Thromboembolism affects 28-50% of Covid-19 patients in the ICU, resulting in significant morbidity and mortality.22,95 These appear to be cases of anti-phospholipid syndrome, which is often directly related to low vitamin D.22 Microcirculatory dysfunction in patients with severe Covid-19 appears to be related to endotheliopathy.96 Endothelium destabilization by inflammatory cytokines, found in hypertension, diabetes mellitus, chronic renal failure, atherosclerosis, and many other inflammatory diseases, causes dysregulated clotting.6,91 All of these conditions are associated with low levels of vitamin D, which is known to stabilize the endothelium.6,16 Vitamin D supplementation has successfully corrected high levels of inflammatory cytokines, including TNF-a, IL-6, and CRP.83,91 Vitamin D’s induction of LL37 would lead to decreased expression of inflammatory IL17, which is abnormally high in Covid-19 and can lead to thrombosis and ARDS.32 Low vitamin D is also implicated in higher levels of cellular adhesion molecules.91 Vitamin D supplementation has been shown to decrease thrombus formation directly in high risk patients.91
A recent study demonstrated that inadequate vitamin D levels can result in a poor immune response to vaccines in elderly individuals, which has clear implications for recommendations during the Covid-19 pandemic.97
Correlational evidence regarding serum vitamin D levels and Covid-19 outcomes
As early as February, 2020, experts were presenting evidence to support the hypothesis that low vitamin D has a dramatic influence on Covid-19 outcomes.98 It was clear that the populations with the worst Covid-19 outcomes are the exact same populations who tend to have the lowest vitamin D levels: the elderly, males, people with metabolic syndrome-related illnesses like diabetes, obesity, hypertension, and kidney failure, people whose area had just experienced winter, and people with melanin-rich skin who do get not consistent exposure to the tropical sun.16
Dramatically, of the first 10 physicians in the UK to die of Covid-19, all had naturally melanin-rich skin, and by the time 119 NHS staff had succumbed, the fact that people with melanin-rich skin living outside the tropics are at much higher risk was undeniable in the USA, as well.99,100 On 29 April 2020 a communication went out to all “BAME” working doctors in England and Wales, warning them that they could be at high risk for Covid-19 due to vitamin D deficiency, and urging supplementation, including a high loading dose: three days later, the deaths in this group came to an abrupt end.101 Meanwhile, despite poverty and poor health infrastructure, Africans living in the tropics have still not succumbed in large numbers.102 Ockham’s Razor, “Do not multiply entities without necessity” (The simplest explanation is likely to be true) would appear to apply.103
For some vitamin D experts, a devastating viral pandemic had been anticipated; they had long been watching the immune systems of populations around the world become increasingly dysregulated due to lower vitamin D levels, particularly in winter.60,104,105 Eerily, every symptom of severe Covid-19 could be explained by inadequate vitamin D.16 Their strong response (there were already 181 scholarly works on the topic by mid-June, 2020) was to document what appeared to be a clear relationship between lower vitamin D levels and worse Covid-19 outcomes in order to persuade public health authorities to support widespread supplementation 16. This early documentation came primarily in the form of biological plausibility presentations, population (geographical) evidence analyses, prospective correlational studies, and retrospective chart reviews (see links at www.vitaminDforAll.org).16,106 (Figure 4, page 10)
These forms of evidence have increased daily. Today, in addition to the earlier evidence types, some intervention studies and dozens of meta-analyses and systematic reviews on the relationship between vitamin D levels and Covid-19 can be found with a quick PubMed search. Only a few examples are detailed here.
Figure 4: Early study demonstrating a dramatic correlation between lower vitamin D levels and worse Covid-19 outcomes.
Evidence based population data (geographical, ecological)
Pugach and Pugach evaluated recent reliable data on the country-wide prevalence of vitamin D deficiency in 10 European countries, finding a statistically significant and linear relationship between prevalence of vitamin D deficiency and deaths/million from Covid-19.107 Adjusting for the countries’ age structure and health expenditures, each 1% increase In severe vitamin D deficiency increased deaths from Covid-19 by 55/million.107
Walrand challenged the widely held belief that Covid-19 cases increase in winter due to cooler temperatures.108 Using automatic fitting software to compare case data for 18 countries against temperature and UV radiation (adjusted for latitude and time of year) 2 weeks prior, he determined that the autumn 2020 “surge” in Covid-19 cases in Europe was completely unrelated to temperatures but was significantly related to decreased sunshine, and predicted that the crisis would continue until spring (which it did).108,109
A group of Italian researchers led by Isaia and Diemoz noted that despite uniform exposure prevention measures throughout the country, the Covid-19 pandemic hit northern Italy much harder than it hit southern Italy.110 A literature search for potential environmental causes yielded UVB for its ability to increase population vitamin D levels.110 Taking into account air quality, they calculated the UVB exposure for residents in each of the 20 regions from June-Dec 2019: the time leading up to the pandemic.110 They also compared air temperature, relative humidity, population age, percentage in nursing homes, and potentially relevant comorbidities.110 Univariate regression found that 74.2% of the variation in Covid-19 fatalities between districts and 41.4% of the variation in cases between districts was explained by vitamin D producing UV light in the preceding months, far more than any other parameter.110
A group led by Jayawardena compared population vitamin D deficiency prevalence from the past 10 years (mostly in the past 5 years) with Covid-19 cases and fatalities per million in 24 countries in Asia, an area with dramatically divergent Covid-19 outcomes, as of Dec 31, 2020.111 Vitamin D deficiency, defined as 25(OH)D<20ng/ml affected over 50% of the adults in three- fourths of these countries, in part due to customs which limit sunlight exposure.111 Covid-19 cases/million population and fatalities/million were positively correlated with the prevalence of vitamin D deficiency (cases: r=0.55, p=0.01; fatalities: r=0.50, p=0.01).111 The variation of total cases and total fatalities can be attributed to vitamin D deficiency at proportions of 33% for cases and 25% for fatalities.111
Evidence based on individual data (chart reviews)
Early chart reviews demonstrating that lower vitamin D levels were correlated with worse Covid-19 outcomes were criticized because it is known that illness can cause vitamin D levels to decline.4,112 Although this decline would not explain the dramatic differences some of these studies found,112 more recent studies often use vitamin D levels taken weeks or months prior to infection to eliminate this confounder. The four such studies summarized here all corroborate the conclusions of earlier researchers.
Merzon’s group in Israel found that over half (7807) of the 14,022 patients in their health maintenance organization’s database who were tested for Covid-19 in Feb-April of 2020 had a previous 25(OH)D level on file.113 The proportion who tested positive was the same for those with and those without recorded vitamin D levels.113 After controlling for demographic, psychiatric, and somatic variables, multivariate analysis demonstrated a significant and independent association between 25(OH)D below 30ng/ml and positive PCR results [1.45 (95% CI: 1.08-1.95, p<0.001)].113 Plasma 25(OH)D under 20mg/ml almost doubled the risk of hospitalization due to Covid-19.113
Researchers accessed a de-identified laboratory database with 191,779 patients from all 50 US states who had both PCR tests for Covid-19 and 25(OH)D levels from the preceding 12 months, using zip code data to determine race/ethnicity proportions and latitude.50 Patients with seasonally adjusted 25(OH)D levels below 20ng/ml were significantly more likely to test positive for Covid-1950 and those with levels >55ng/ml were the least likely to test positive.50 A multivariate logistic model demonstrated that the relationship is robust, remaining significant (ORadj 0.984 per ng/mL increment, 95% C.I. 0.983-0.986; p<0.001) when adjusted across latitudes, race/ethnicity, sex, and age ranges.50
A large Chicago-based medical center database was mined for a relationship between vitamin D levels within the previous year and positive Covid-19 test results as of Dec 30, 2020.114 Treatment for deficiency was factored into the results to provide an estimate of concurrent vitamin D levels.114 A total of 4638 individuals were included in the study, of whom 48% were black.114 Black patients had significantly lower vitamin D levels than did white patients.114 Of the 333 patients with Covid-19 positive tests, over two-thirds were black.114 Multivariate analysis found that a negative Covid-19 test was associated with vitamin D level >30ng/ml (IRR 0.97 (95% CL=0.94-0.99; P=0.008) per 1-ng/ml increase in vitamin D) with an even greater effect in black patients.114 The authors found that 40ng/ml, rather than 30ng/ml, was the level at which vitamin D became significantly protective against Covid-19, leading them to recommend supplementation with 10,000 IU of vitamin D3/day.114
Using a 987,849 patient database in Florida, Katz, Yue, and Xue searched ICD 10 codes for Covid-19 patients for vitamin D deficiency, diabetes, obesity, malabsorption, and dental diseases diagnosed in the previous 5 years.115 The researchers found that 887 had a Covid-19 diagnosis, 31950 had vitamin D deficiency, and 87 had both.115 Those with both were more likely to be male, and only 12% were white.115* Vitamin D deficient patients were 4.6 times more likely to test Covid-19 positive than patients without this diagnosis. *115 The association remained highly significant (p<0.001) even after controlling for all comorbidities.115 After adjusting for age, it was determined that patients diagnosed as vitamin D deficient were 5 times more likely to be infected with SARS-CoV-2 as those without this diagnosis (OR=5.155) 95% CI 3.974-6.688, P<0.001).115
Evidence based on meta-analyses and systematic reviews
At least 26 systematic and basic review and meta-analysis papers on the topic of the relationship between Covid-19 outcomes and vitamin D levels have been published to date (see Table 1, pages 18-19).
An early meta-analysis of 10 case control studies found, in the pooled analysis, that vitamin D deficiency or insufficiency, defined as 25(OH)D < 30ng/ml, significantly increased the odds of contracting Covid-19 (OR=1.43,95%, CI=1.00-2.05).116 In addition, the average vitamin D level of Covid-19 positive groups was significantly lower than that of negative groups (SMD=-0.37,95% CI=-0.52 to -0.21, I2=89.6%).116
Oscanoa’s group evaluated the 23 observational studies published by the end of 2020 to determine the relationship between Covid-19 severity and mortality and vitamin D levels.4 Pooled results demonstrated that vitamin D deficiency is associated with significantly increased risks of poor Covid-19 outcomes, with 17 studies addressing severe Covid-19 (RR 2.00; 95% CL=1.47-2.71) and 13 addressing mortality (RR 2.45; 95% CL=1.24-4.84).4
The first meta-analysis to include only intervention studies which all had a very low risk of bias found that vitamin D supplementation clearly decreases Covid-19 mortality (pooled OR=0.264, 95% CI=0.099-0.708, p=0.008) and two studies demonstrated a significant (p=0.001) decrease in OSCI severity scores.117 The four studies included in this analysis will be further discussed in the next section.
A large rigorous meta-analysis of studies examined 39 cohort, randomized controlled trials, and cross-sectional studies as of 26 Nov 2020, excluding all preprints.31 ORs and CIs were reported for each outcome by pooling studies based upon the statistical adjustments used by the authors.31 Kazemi, et al., found that vitamin D was strongly associated with Covid-19 mortality and severity, and is also likely a factor in infection rates, although those study designs were less strong.31 The evidence for decreasing inflammatory markers and hospital, ICU, and ventilator utilization was less clear.31 In one study, the probability of a fatal outcome was ten times higher if 25(OH)D was less than 10ng/ml than if it was more than 10ng/ml.31,118
Authors of a June 2021 meta-analysis of 13 vitamin D intervention studies that reported ICU admissions, severity and/or fatality rates for Covid-19 patients found that cholecalciferol (11 studies) or calcifediol (2 studies) supplementation significantly reduced risk of ICU admissions/mortality (pooled OR 0.41, 95% CL=0.20, 0.81, p=0.01, I2=66%, random-effects model) and adverse outcomes (pooled OR 0.27, 95% CL= 0.08, 0.91, p=0.03, 2I=80%, randomeffects model).32
A meta-analysis in July 2021 found 13 RCTs, quasi-RCTs and observational studies meeting the authors’ quality criteria which included individual vitamin D levels upon testing for infection. The researchers determined that low 25(OH)D is statistically significantly associated with risk of Covid-19 infection, recommending supplementation for high risk and deficient groups.119 Another meta-analysis published in June evaluated 23 studies both qualitatively and quantitatively, finding that Covid-19 patients all had low mean 25(OH)D levels, and D deficiency was associated with a 3x higher risk of infection and 5x higher risk of severe Covid- 19.120
The clear consensus of these meta-analysis authors is that there is a strong relationship between vitamin D levels and Covid-19 outcomes. The studies reviewed demonstrated that vitamin D supplementation and/or higher vitamin D levels are associated with decreased chances of developing Covid-19 infection; decreased chance of developing severe Covid-19; decreased chance of requiring oxygen, hospitalization, ICU care, or mechanical ventilation; and decreased chance of death due to Covid-19 (see Table 1, pages 18-19). Vitamin D supplementation is also associated with a decrease in fibrinogen, an inflammatory marker.78
Despite this powerful evidence, public health officials continued to call for randomized controlled trials. The question of causation had to be addressed, particularly for those unfamiliar with the biological plausibility of the relationship.
Evidence that vitamin D is a causal factor in poor Covid-19 outcomes
Calls for randomized controlled trials to prove a causal relationship cannot, however, be heeded by most vitamin D experts. Vitamin D is not a novel drug which may or may not be beneficial, but rather, it is known to be essential to human health. A scientist who believes that low vitamin D levels are responsible for high mortality rates cannot ethically withhold this lifesaving substance from the placebo group.121,122
Early causal modeling studies
This ethical dilemma was solved in 1965 by Sir Bradford Hill, who developed a causal model to demonstrate that smoking is a cause of lung cancer. Hill’s criteria were used to demonstrate that low vitamin D is a cause of severe Covid-19 in a MEDLINE indexed article in May of 2020.123 Vitamin D met all but one of Hill’s criteria, specificity, which it failed only because vitamin D deficiency is ubiquitous.123 Later authors concurred that the evidence to date satisfied Hill’s criteria (strength of association, consistency, temporality, biological gradient, plausibility, and coherence), clearly demonstrating causality.83
The idea that robust vitamin D levels are merely a marker for good health (a “bystander”) has persisted in part because sick people are less likely to spend time outdoors, and because vitamin D is consumed in slightly higher quantities during illness. Davies, Garami, & Byers noticed a strong relationship between early Covid-19 fatalities and latitude.124 This observation led them to create a causal inference framework specific to testing the vitamin D hypothesis.124 The model produced strong evidence that Vitamin D was a cause of Covid-19 fatalities, and moderate evidence for vitamin D causing cases, with causation fitting the data for 16 predictions.124 The bystander model for vitamin D was strongly contradicted by the data for 14 predictions.124
Intervention studies
Calls for RCTs continued, and several have been conducted. However, the study designs often reveal a lack of insight into how vitamin D is utilized by the body. Giving oral cholecalciferol to patients who already have severe Covid-19 is clearly unlikely to be effective (see section IIA, pages 3-4, Defining vitamin D). In addition, the response curve for vitamin D is S-shaped, not linear.121,125 Therefore, providing vitamin D to individuals whose levels are already replete will not demonstrate a benefit, and giving inadequate doses to people who are severely deficient may not bring their levels up high enough to provide immune benefits.121,125 Because either of these common scenarios can make an intervention that could be life-saving for people whose vitamin D levels are in between these extremes appear ineffective, and because individual supplementation response is influenced by genetics, obesity, diabetes, etc., trials must be guided by participant 25(OH)D levels.16,125,126
Vitamin D requirements for immune health are far higher than those for bone health.16,58 Virtually any medication can be “proven” ineffective by a study in which only 1/10 the required dose is given. Dosing intervals are also of critical importance in vitamin D trials; studies have shown that large infrequent boluses can prevent the formation of new calcifediol for at least 28 days, and are instead broken down by the body relatively quickly, with the by product, calcitroic acid, being indistinguishable from active calcifediol to most 25(OH)D tests.36,37,41,74,122,127 Finally, in recent Covid-19 trials, some large-seeming studies had relatively few participants who were actually exposed to SARS-CoV-2 during the study period.128
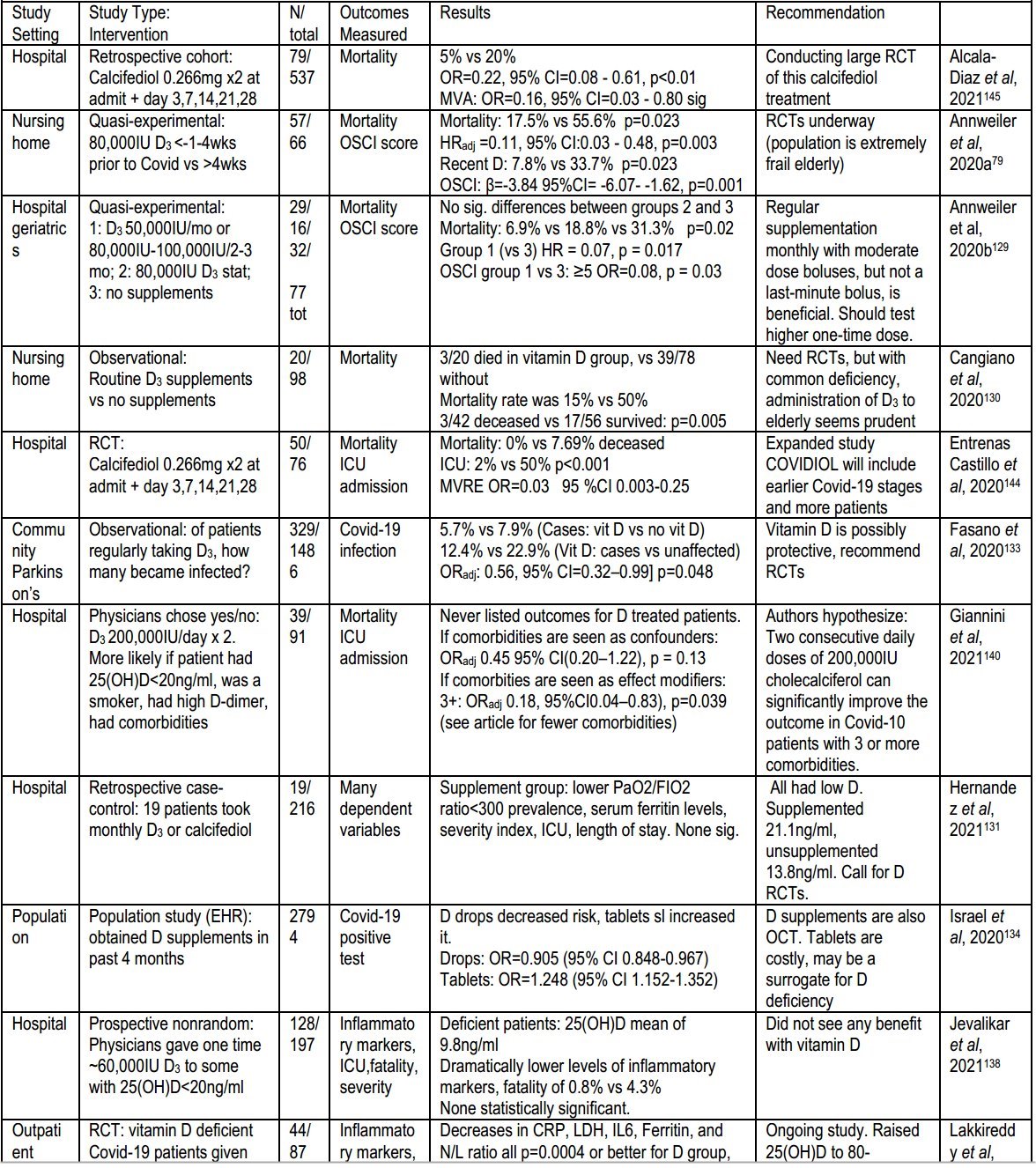
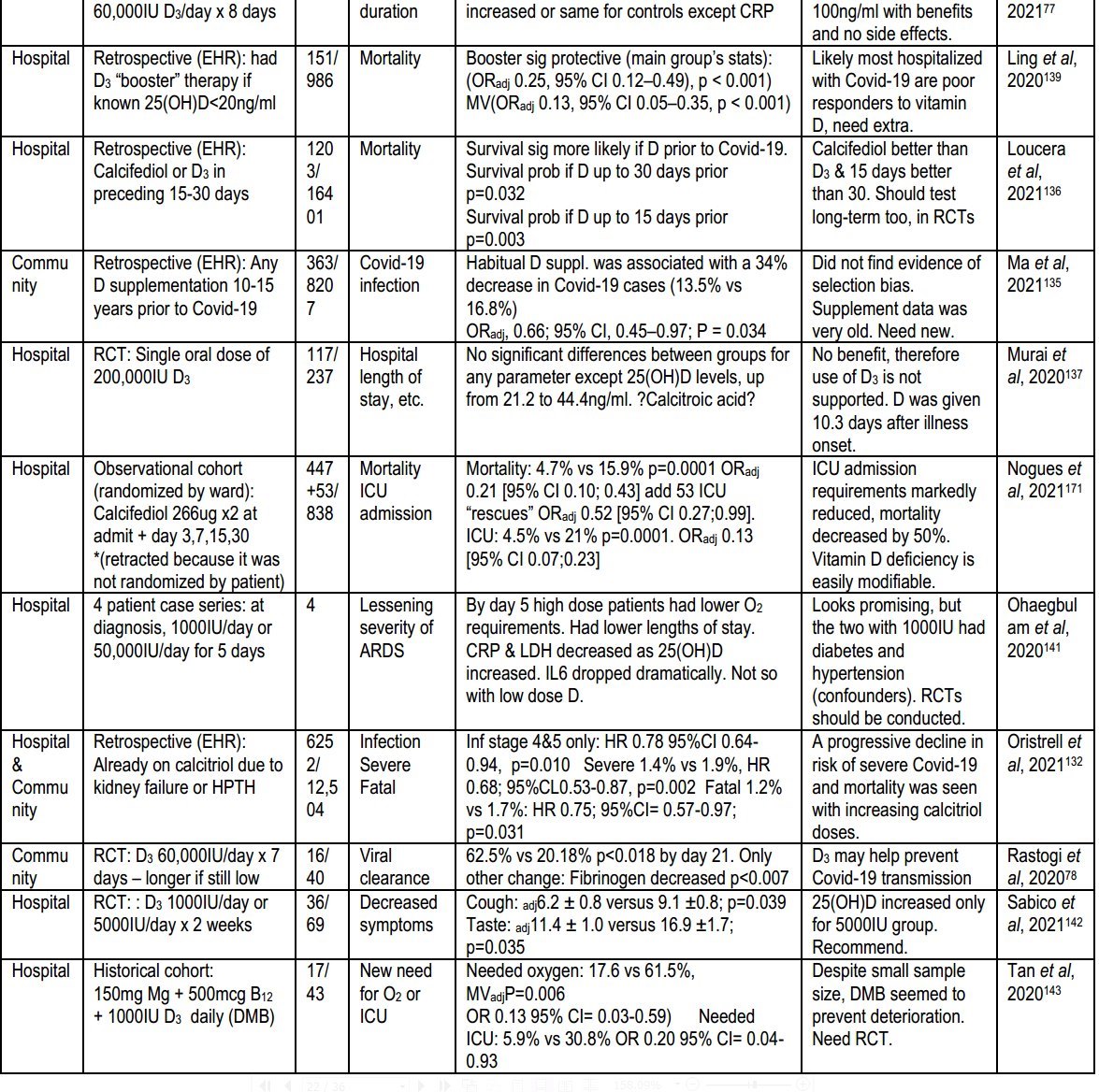
Beginning in late 2020, an increasing number of innovative intervention studies were published demonstrating a clear causal relationship between low vitamin D levels and worse Covid-19 outcomes. (See Table 2, pages 20-21, for summaries of these studies as of June 2021, along with odds ratios, hazard ratios, confidence intervals, and other statistical findings.)
Several researchers evaluated Covid-19 outcomes for individuals who were already supplementing with vitamin D. Annweiler published two quasi-experimental studies which found that if frail elderly people in long term care or in a hospital geriatric ward had been given a cholecalciferol bolus (50,000-80,000 IU) more recently, their subsequent cases of Covid-19 were statistically significantly less likely to be as severe when compared with their counterparts who had not had the supplemental D3 as recently.79,129 Both studies also found that the recently supplemented frail elderly patients were over three times less likely to die than those who did not receive supplements recently.79,129 Cangiano’s team found that, when compared with no vitamin D supplements, routine vitamin D3 supplements of any kind also decreased the risk of Covid-19 mortality in nursing home residents to less than a third that of the unsupplemented group.130
In a study in which only 19 hospitalized patients had a history of any vitamin D supplementation (usually monthly) and 82% of the patients had very low 25(OH)D levels on admission (mean 13.8ng/ml), Hernandez, et al., found that vitamin D seemed to improve several indicators of Covid-19 severity, but none reached statistical significance.131
Oristrell compared the electronic health records (EHR) of 6252 patients who were on calcitriol for severe kidney disease or hypoparathyroidism with matched controls, finding a significant (p=0.002) and progressive decline in risk of severe Covid-19 with increasing doses of calcitriol.132 End stage renal disease patients were also significantly less likely to have become infected with Covid-19 (p=0.010).132 The likelihood of fatal Covid-19 was decreased (p=0.031) for all patients taking calcitriol.132
During the height of the Covid-19 pandemic, Fasano’s group conducted telephone interviews of 1486 Parkinson’s patients who had attended their practice, finding that the 329 who regularly took cholecalciferol supplements were about half as likely to have tested positive for Covid-19.133
Two groups of researchers mined large EHR databases to explore the relationship between vitamin D supplement prescriptions and testing positive for Covid-19.134,135 Ma, et al., looked at 8207 records from over 10 years prior to the pandemic, while Israel looked at 2794 records from within 4 months of testing.134,135 Ma, et al., found that “habitual” vitamin D supplementation was associated with a 34% decrease in Covid-19 cases, while Israel et al., found that recent supplementation with vitamin D3 drops decreased Covid-19 cases, but not with tablets, perhaps because the tablets were so costly that they were likely to be prescribed only to patients with severe vitamin D deficiency.134,135
Loucera, et al., mined a database with 16401 hospitalized Covid-19 patients to see if the 1203 who were prescribed vitamin D supplements in the 15 or 30 days prior to their hospitalization were more likely to survive than those who were not prescribed D.136 They found a significant reduction in mortality, which was larger if the form of vitamin D was calcifediol or the prescription was only 15 days prior to hospitalization p=0.003).136
Two research groups in India each gave 60,000 IU/day of cholecalciferol to outpatients who tested positive for Covid-19 and compared their inflammatory marker levels with controls.77,78 Lakkireddy, et al., found that vitamin D3 decreased CRP, LDH, IL-6, Ferritin, and the N/L ratio with a significance of p=0.0004 or better, while in the control group several of these markers increased and only CRP levels improved.77 Rastogi, et al., found that in the D3 supplemented group fibrinogen decreased more quickly (p=0.007) and that three times as many in the treatment group achieved Covid-19 PCR test negativity by day 21 (62.5% vs 20.8%, p=0.018).78 The more rapid viral clearance was expected to result in less chance of spreading Covid-19 and a more rapid return to work.78
Patients were given a one-time large dose of cholecalciferol after hospitalization for Covid-19 in three studies. - In two of these intervention studies plus a third in which lesser doses of cholecalciferol were given at regular intervals, patients with 25(OH)D levels less than 20ng/ml were more likely to receive supplementation.138-140 It is quite possible that many of these patients subsequently enjoyed higher 25(OH)D levels than some of the initially "vitamin D sufficient" patients.138-140 In a fourth study, the one-time large dose of cholecalciferol was given an average of 10.3 days after symptom onset.137 It is likely that much of the cholecalciferol given to seriously ill patients in these four studies was immediately broken down into calcitroic acid and that calcifediol levels were actually depressed as a result of the boluses.36,37,41 Despite this concern, none of the treatment groups fared worse than the controls.137-140 The researchers who gave lesser doses of cholecalciferol at regular intervals found that this treatment led to significantly (p=0.001) fewer mortalities when compared with unsupplemented patients.139
Two research groups compared D3 supplementation at 1000 IU/day with a higher daily dose in hospitalized Covid-19 patients to evaluate the differences in severity of symptoms.141,142 In a case series with four patients, Ohaebulam, et al., found that 50,000 IU/day led to shorter lengths of stay, lower oxygen requirements, decreased CRP and LDH, and a dramatic drop in IL- 6 compared with patients who received 1000 IU/day, whose 25(OH)D levels did not increase.141 The second study was a 69 patient randomized controlled trial in which, again, 25(OH)D levels did not increase for the 1000 IU/day group.142 These researchers found that 5000 IU/day for two weeks led to significantly quicker resolution of cough (p=0.039) and loss of taste (p=0.035).142
A historical cohort study compared previously treated hospital patients with the next 17 patients, who were managed with the same treatment protocols, but with the addition of 1000 IU D3 + 500mcg B12 + 150mg magnesium (DBM) daily, assessing for new need for oxygen or ICU care.143 New oxygen need decreased from 61.5% to 17.6% (multivariate-adjusted p=0.006), and the need for ICU care decreased from 30.8% to 5.9%.143 The authors called for a randomized controlled trial of their DBM treatment protocol.143
In an anecdotal published report, physicians at the Iranian Hospital in Dubai, UAE described their Covid-19 vitamin D supplementation protocol, which is individualized according to the patient’s weight and 25(OH)D level.59 Asserting that typical endocrine societies guidelines suggest that 40-60ng/ml is the ideal 25(OH)D level, they routinely aggressively supplement with 70-100IU of D3 per kg per day in their neuro-ophthalmology department without any cases of toxicity.59 Finding that, despite their high risk, none of their patients who contracted Covid-19 had a severe case, they recommended this dosage plus an initial bolus of 300,000 IU IM for all Covid-19 admissions, which they report resulted in the ICU being completely cleared of Covid- 19 patients.59
Researchers for three studies conducted in several hospitals in Spain addressed the problem of slow metabolism of cholecalciferol by giving patients moderately high doses of calcifediol early in their hospitalization and at regular intervals.144-147 This protocol consistently resulted in a dramatic decline in ICU admissions and mortality rates. In the pilot study, the ICU admission rate for the treated patients was 2% with no fatalities, compared with a 50% ICU admission and 7.7% fatality rate for the untreated patients.144 A second trial of the same calcifediol protocol resulted in a decrease in fatalities from 20% for the control group to only 5% in the treatment group.145 The third study resulted in 4.5% of the vitamin D supplementation group being admitted to ICU, compared with 21% in the control group.146 In 53 cases, physicians believed that an ICU patient in the control group might be rescued by giving them calcifediol.146 Mortality for the original study groups was 4.7% for the treatment group and 15.9% for the control group.146 If the 53 control group patients who received calcifediol only after being admitted to the ICU are added to the treatment group, the mortality for the treatment group increases to 7.2% and mortality for the control group decreases to 13.9% (p=0.001).146 The researchers noted that the patients who died had lower baseline 25(OH)D levels (9ng/ml) than the ones who survived (13ng/ml).146
These intervention studies all strongly support the hypothesis that low serum calcifediol levels are a significant causal factor in poor Covid-19 outcomes.
Future Research Opportunities
Several of the research studies described above show enough promise that expanding upon them is likely to be beneficial. In addition, much more needs to be learned about the relationship between supplementation and calcifediol levels.
Research priorities during the Covid-19 pandemic are:
A rigorous, multi-center study of the calcifediol supplementation protocol used in the three highly successful Spanish studies for hospitalized Covid-19 patients
A longitudinal study comparing individuals who take daily D3 supplements at various doses to determine the optimal usual dose based upon percent body fat
A large EHR study of individuals with 25(OH)D levels taken within the past year, comparing Covid-19 infection, hospitalization, ICU admission, and fatality rates between those with levels over 50ng/ml and those the levels that are 20-30ng/ml.
Specific recommendations for Vitamin D supplementation to improve Covid-19 outcomes
Several groups of experts have called for widespread vitamin D supplementation to help prevent poor Covid-19 outcomes. The largest group is VitaminDforAll.org, a coalition representing 220 professors, medical doctors, and PhD vitamin D experts from 33 countries.106 Every signatory recommends universal supplementation with 4000 IU/day of vitamin D3 (or at least 2000 IU/day) in the absence of testing, with the goal of raising 25(OH)D levels to at least 30ng/ml.106 Those at especially high risk for deficiency (due to weight, frailty, dark skin) are encouraged to consider doubling that dose.106 Individuals who have not previously taken vitamin D supplements should take D3 10,000 IU/day for 2-3 weeks initially, or until serum 25(OH)D levels can be drawn, then drop to the above amounts.106
The Italian Academy of Medicine of Turin letter, signed by a group of 152 Italian professors and physicians, also calls for universal supplementation with D3 4000 IU/day, but with a goal of acquiring 25(OH)D levels of 40ng/ml.148 The French La Revue du Praticien, signed by 73 French authors with the support of 6 national scientific societies, calls for prophylaxis with D3 of 1200IU/day, or double that amount for obesity, noting that 4000 IU/day is safe.149 The Health Committee of the Legislature of Ireland (Oireachtas) recommends daily vitamin D supplementation of 800-1000 IU for the entire adult population, with higher doses for vulnerable groups, along with public education and encouragement, including reducing the cost and making supplementation an opt-out.150,151
The vitaminDforAll.org coalition and Italian Academy of Medicine of Turin letter both recommend that all hospitalized Covid-19 patients have 25(OH)D levels drawn upon admission and be treated with calcifediol or D3, using a protocol for calcifediol such as the one the three Spanish trials used so successfully or the cholecalciferol 60,000 IU/day used successfully by Rastogi, et al.106,148 The French La Revue du Praticien recommends D3 100,000 IU upon diagnosis, to be repeated 7 days later.149* Based upon the totality of the evidence, the vitaminDforAll.org recommendation: ** 4000 IU per day as maintenance for all adults without medical contraindications
- 10,000 IU/day for 2-3 weeks initially for those not previously supplemented adjusted to meet a goal serum 25(OH)D of at minimum 30ng/ml should be safe (all studies support this), and is the most likely to be effective.
Table 1 - Summary of Systematic and Basic Reviews and Meta-analyses Specific to Covid-19 and Vitamin D
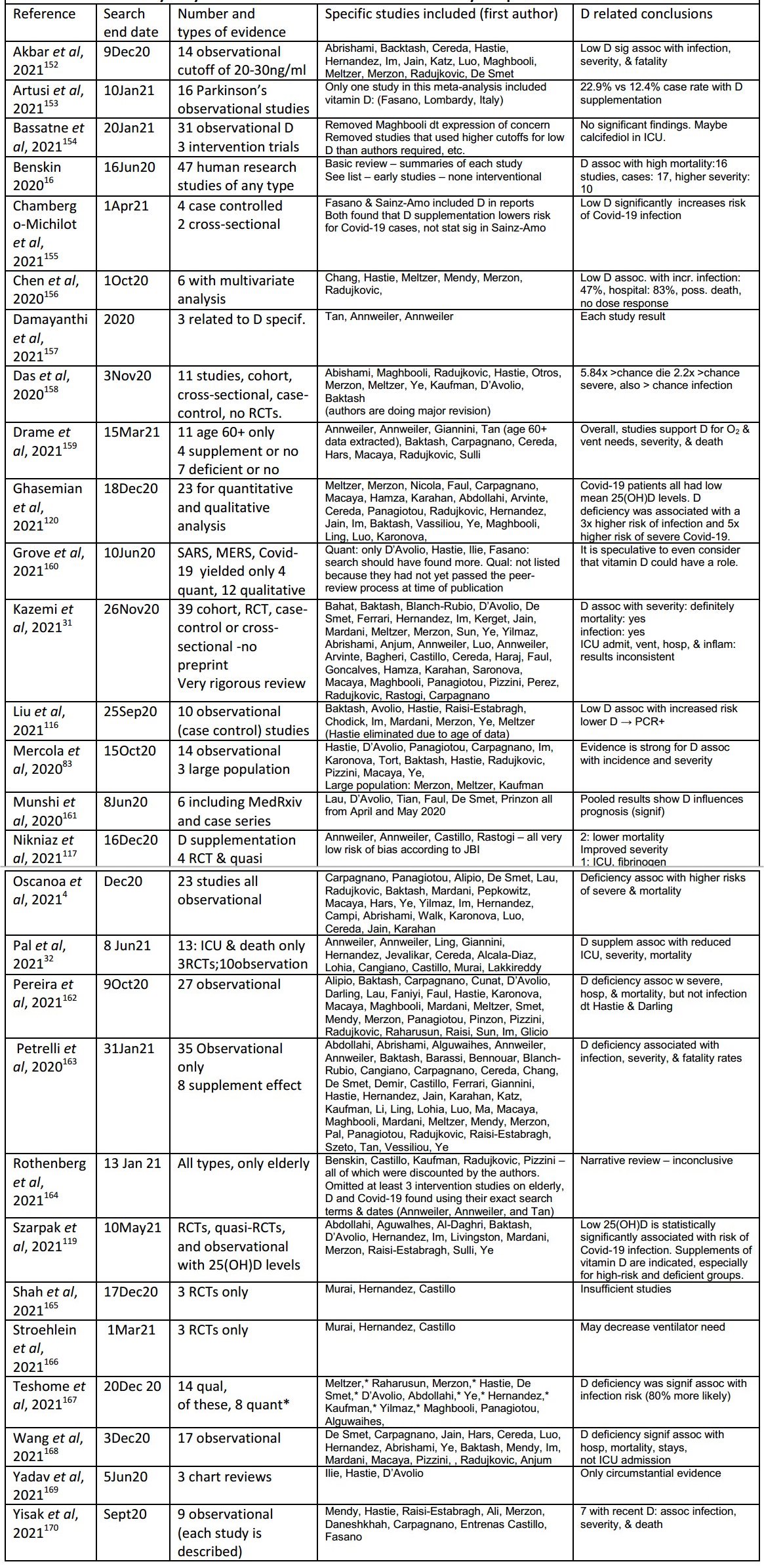
Table 2 Intervention
REFERENCES
Norval M. A Short Circular History of Vitamin D from its Discovery to its Effects. Res Medica [Internet]. 2005 [cited 2021 Jun 8];268(2). Available from: http://journals.ed.ac.uk/resmedica/article/view/1031
Wolf G. The Discovery of Vitamin D: The Contribution of Adolf Windaus. The Journal of Nutrition [Internet]. 2004 Jun 1 [cited 2021 Jun 29];134(6):1299-302. Available from: https://doi.org/10.1093/jn/134.6T299
Hollis BW, Wagner CL. The Role of the Parent Compound Vitamin D with Respect to Metabolism and Function: Why Clinical Dose Intervals Can Affect Clinical Outcomes. J Clin Endocrinol Metab [Internet]. 2013 Dec [cited 2021 Jun 25];98(12):4619-28. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3849670/
Oscanoa TJ, Amado J, Vidal X, Laird E, Ghashut RA, Romero-Ortuno R. The relationship between the severity and mortality of SARS-CoV-2 infection and 25-hydroxyvitamin D concentration — a metaanalysis. Advances in Respiratory Medicine [Internet]. 2021 [cited 2021 May 10];89(2):145-57. Available from: https://journals.viamedica.pl/advancesinrespiratory_medicine/article/view/ARM.a2021.0037
Mailhot G, White JH. Vitamin D and Immunity in Infants and Children. Nutrients [Internet]. 2020 Apr 27 [cited 2021 Jun 10];12(5). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7282029/
Gibson CC, Davis CT, Zhu W, Bowman-Kirigin JA, Walker AE, Tai Z, et al. Dietary Vitamin D and Its Metabolites Non-Genomically Stabilize the Endothelium. PLOS ONE [Internet]. 2015 Oct 15 [cited 2021 Jun 24];10(10):e0140370. Available from:
https://journals.plos.org/plosone/article7idM0.1371/journal.pone.0140370
Charoenngam N, Holick MF. Immunologic Effects of Vitamin D on Human Health and Disease. Nutrients [Internet]. 2020 Jul [cited 2021 Jun 12];12(7):2097. Available from: https://www.mdpi.com/2072- 6643/12/7/2097
Rybchyn MS, Abboud M, Puglisi DA, Gordon-Thomson C, Brennan-Speranza TC, Mason RS, et al.
Skeletal Muscle and the Maintenance of Vitamin D Status. Nutrients [Internet]. 2020 Nov [cited 2021 Aug 20];12(11):3270. Available from: https://www.mdpi.com/2072-6643/12/11/3270
Martinaityte I, Kamycheva E, Didriksen A, Jakobsen J, Jorde R. Vitamin D Stored in Fat Tissue During a 5- Year Intervention Affects Serum 25-Hydroxyvitamin D Levels the Following Year. The Journal of Clinical Endocrinology & Metabolism [Internet]. 2017 Oct 1 [cited 2021 Jun 25];102(10):3731-8. Available from: https://doi.org/10.1210/jc.2017-01187
Hyppönen E, Boucher BJ. Avoidance of vitamin D deficiency in pregnancy in the United Kingdom: the case for a unified approach in National policy. British Journal of Nutrition [Internet]. 2010 Aug [cited 2021 Jun 24];104(3):309-14. Available from: https://www.cambridge.org/core/journals/british-journal-of- nutrition/article/avoidance-of-vitamin-d-deficiency-in-pregnancy-in-the-united-kingdom-the-case-for-a- unified-approach-in-national-policy/B13CC21188F1FF9C67486629518DA20F
Scully H, Laird E, Healy M, Walsh JB, Crowley V, McCarroll K. Geomapping Vitamin D Status in a Large City and Surrounding Population—Exploring the Impact of Location and Demographics. Nutrients [Internet]. 2020 Aug 31 [cited 2021 Jun 24];12(9):2663. Available from:https ://www. ncbi.nlm.nih. gov/pmc/articles/PMC7551618/
Quraishi SA, Bittner EA, Blum L, Hutter MM, Camargo CA. Association Between Preoperative 25 - Hydroxyvitamin D Level and Hospital-Acquired Infections Following Roux-en-Y Gastric Bypass Surgery.
JAMA Surg [Internet]. 2014 Feb 1 [cited 2021 Jun 1];149(2):112. Available from: http://archsurg.jamanetwork.com/article.aspx7doiM0.1001/jamasurg.2013.3176
Grant WB, Baggerly CA, Lahore H. Reply: “Vitamin D Supplementation in Influenza and COVID-19 Infections. Comment on: Evidence That Vitamin D Supplementation Could Reduce Risk of Influenza and COVID-19 Infections and Deaths Nutrients 2020, 12(4), 988.” Nutrients [Internet]. 2020 Jun [cited 2020 Jun 16];12(6):1620. Available from: http://www.mdpi.com/2072-6643/12/6/1620
Griffin G, Hewison M, Hopkin J, Kenny RA, Quinton R, Rhodes J, et al. Preventing vitamin D deficiency during the COVID-19 pandemic: UK definitions of vitamin D sufficiency and recommended supplement dose are set too low. Clinical Medicine [Internet]. 2020 Nov 6 [cited 2020 Nov 6]; Available from: https://www.rcpjournals.org/content/clinmedicine/early/2020/11/06/clinmed.2020-0858
Lu Z, Chen TC, Zhang A, Persons KS, Kohn N, Berkowitz R, et al. An Evaluation of the Vitamin D3 Content in Fish: Is the Vitamin D Content Adequate to Satisfy the Dietary Requirement for Vitamin D? J Steroid Biochem Mol Biol [Internet]. 2007 Mar [cited 2021 Jun 9];103(3-5):642-4. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2698592/
Benskin LL. A Basic Review of the Preliminary Evidence That COVID-19 Risk and Severity Is Increased in Vitamin D Deficiency. Front Public Health [Internet]. 2020 Sep 10 [cited 2020 Sep 11];8:513. Available from: https://www.frontiersin.org/article/10.3389/fpubh.2020.00513/full
Ames BN, Grant WB, Willett WC. Does the High Prevalence of Vitamin D Deficiency in African Americans Contribute to Health Disparities? Nutrients [Internet]. 2021 Feb [cited 2021 Feb 3];13(2):499. Available from: https://www.mdpi.com/2072-6643/13/2/499
Holick MichaelF, Matsuoka LoisY, Wortsman J. AGE, VITAMIN D, AND SOLAR ULTRAVIOLET. The Lancet [Internet]. 1989 Nov 4 [cited 2020 Apr 23];334(8671):1104-5. Available from: http://www.sciencedirect.com/science/article/pii/S0140673689911240
Kara M, Ekiz T, Ricci V, Kara Ö, Chang K-V, Ôzçakar L. “Scientific Strabismus” or two related pandemics: coronavirus disease and vitamin D deficiency. Br J Nutr. 2020 Oct 14;124(7):736-41.
Cashman KD, Dowling KG, Skrabakova Z, Gonzalez-Gross M, Valtuena J, De Henauw S, et al. Vitamin D deficiency in Europe: pandemic? Am J Clin Nutr. 2016 Apr;103(4):1033-44.
Docea AO, Tsatsakis A, Albulescu D, Cristea O, Zlatian O, Vinceti M, et al. A new threat from an old enemy: Re-emergence of coronavirus (Review). Int J Mol Med [Internet]. 2020 Jun [cited 2020 Jun 22];45(6):1631-43. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7169834/
Rhodes JM, Subramanian S, Laird E, Griffin G, Kenny RA. Perspective: Vitamin D deficiency and COVID- 19 severity - plausibly linked by latitude, ethnicity, impacts on cytokines, ACE2 and thrombosis. Journal of Internal Medicine [Internet]. 2021 [cited 2021 Jun 25];289(1):97-115. Available from: https://onlinelibrary.wiley.com/doi/abs/10.1111/joim.13149
Delorey TM, Ziegler CGK, Heimberg G, Normand R, Yang Y, Segerstolpe Â, et al. COVID-19 tissue atlases reveal SARS-CoV-2 pathology and cellular targets. Nature. 2021 Apr 29;
Cevik M, Kuppalli K, Kindrachuk J, Peiris M. Virology, transmission, and pathogenesis of SARS-CoV-2. BMJ [Internet]. 2020 Oct 23 [cited 2021 Jun 25];371:m3862. Available from:https ://www.bmj .com/content/371/bmj .m3 862
Melms JC, Biermann J, Huang H, Wang Y, Nair A, Tagore S, et al. A molecular single-cell lung atlas of lethal COVID-19. Nature. 2021 Apr 29;
Cevik M, Tate M, Lloyd O, Maraolo AE, Schafers J, Ho A. SARS-CoV-2, SARS-CoV, and MERS-CoV viral load dynamics, duration of viral shedding, and infectiousness: a systematic review and meta-analysis. Lancet Microbe. 2021 Jan;2(1):e13-22.
Gustine JN, Jones D. Immunopathology of Hyperinflammation in COVID-19. Am J Pathol [Internet]. 2021 Jan [cited 2021 Aug 20];191(1):4-17. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7484812/
Andersson MI, Arancibia-Carcamo CV, Auckland K, Baillie JK, Barnes E, Beneke T, et al. SARS-CoV-2 RNA detected in blood products from patients with COVID-19 is not associated with infectious virus. Wellcome Open Res [Internet]. 2020 Oct 12 [cited 2021 Jun 25];5:181. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7689603/
Wölfel R, Corman VM, Guggemos W, Seilmaier M, Zange S, Müller MA, et al. Virological assessment of hospitalized patients with COVID-2019. Nature [Internet]. 2020 May [cited 2021 Jun 25];581(7809):465-9. Available from: https://www.nature.com/articles/s41586-020-2196-x
Saponaro F, Saba A, Zucchi R. An Update on Vitamin D Metabolism. Int J Mol Sci. 2020 Sep 8;21(18).
Kazemi A, Mohammadi V, Aghababaee SK, Golzarand M, Clark CCT, Babajafari S. Association of Vitamin D Status with SARS-CoV-2 Infection or COVID-19 Severity: A Systematic Review and Meta-analysis. Adv Nutr. 2021 Mar 5;
Pal R, Baneijee M, Bhadada SK, Shetty AJ, Singh B, Vyas A. Vitamin D supplementation and clinical outcomes in COVID-19: a systematic review and meta-analysis. J Endocrinol Invest [Internet]. 2021 Jun 24 [cited 2021 Jun 25]; Available from: https://doi.org/10.1007/s40618-021-01614-4
Uday S, Högler W. Nutritional Rickets and Osteomalacia in the Twenty-first Century: Revised Concepts, Public Health, and Prevention Strategies. Curr Osteoporos Rep [Internet]. 2017 [cited 2021 Jun 12];15(4):293-302. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5532418/
Norman AW. From vitamin D to hormone D: fundamentals of the vitamin D endocrine system essential for good health. The American Journal of Clinical Nutrition [Internet]. 2008 Aug 1 [cited 2021 Jun 24];88(2):491S-499S. Available from: https://doi.org/10.1093/ajcn/88.2.491S
3 5. The Body Needs All Forms of Vitamin D [Internet]. GrassrootsHealth. [cited 2021 Jun 25]. Available from:https://myemail.constantcontact.com/The-Body-Needs-All-Forms-of-Vitamin- D.html?soid=1102722411090&aid;=emRzSamZebM
Sosa Henríquez M, Gómez de Tejada Romero MJ. Cholecalciferol or Calcifediol in the Management of Vitamin D Deficiency. Nutrients [Internet]. 2020 May 31 [cited 2021 Jun 24];12(6):1617. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7352679/
Petkovich M, Bishop CW. Chapter 91 - Extended-Release Calcifediol in Renal Disease. In: Feldman D, editor. Vitamin D (Fourth Edition) [Internet]. Academic Press; 2018 [cited 2021 Jun 24]. p. 667-78. Available from: https://www.sciencedirect.com/science/article/pii/B9780128099636000912
Jones KS, Assar S, Harnpanich D, Bouillon R, Lambrechts D, Prentice A, et al. 25(OH)D2 Half-Life Is Shorter Than 25(OH)D3 Half-Life and Is Influenced by DBP Concentration and Genotype. J Clin Endocrinol Metab [Internet]. 2014 Sep [cited 2021 Sep 5];99(9):3373-81. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4207933/
Bouillon R, Bikle D. Vitamin D Metabolism Revised: Fall of Dogmas. Journal of Bone and Mineral Research [Internet]. 2019 [cited 2021 Feb 26];34(11):1985-92. Available from: https://asbmr.onlinelibrary.wiley.com/doi/abs/10.1002/jbmr.3884
Demay MB. The good and the bad of vitamin D inactivation. J Clin Invest [Internet]. 2018 Aug 31 [cited 2021 Jun 23];128(9):3736-8. Available from: https://www.jci.org/articles/view/122046
Ketha H, Thacher TD, Oberhelman SS, Fischer PR, Singh RJ, Kumar R. Comparison of the effect of daily versus bolus dose maternal vitamin D3 supplementation on the 24,25-dihydroxyvitamin D3 to 25- hydroxyvitamin D3 ratio. Bone [Internet]. 2018 May 1 [cited 2021 Jun 29];110:321—5. Available from: https://www.sciencedirect.com/science/article/pii/S8756328218300838
Biondi P, Pepe J, Biamonte F, Occhiuto M, Parisi M, Demofonti C, et al. Oral calcidiol is a good form of vitamin D supplementation. Clin Cases Miner Bone Metab [Internet]. 2017 [cited 2021 Jun 23];14(2):207-8. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5726211/
Navarro-Valverde C, Sosa-Henriquez M, Alhambra-Exposito MR, Quesada-Gomez JM. Vitamin D3 and calcidiol are not equipotent. The Journal of Steroid Biochemistry and Molecular Biology [Internet]. 2016 Nov 1 [cited 2021 Jun 23];164:205-8. Available from: https://www.sciencedirect.com/science/article/pii/S0960076016300140
Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney RP, et al. Evaluation, Treatment, and Prevention of Vitamin D Deficiency: an Endocrine Society Clinical Practice Guideline. The Journal of Clinical Endocrinology & Metabolism [Internet]. 2011 Jul 1 [cited 2021 Aug 20];96(7):1911-30. Available from: https://doi.org/10.1210/jc.2011-0385
Marques CDL, Dantas AT, Fragoso TS, Duarte ÂLBP. The importance of vitamin D levels in autoimmune diseases. Rev Bras Reumatol [Internet]. 2010 Feb [cited 2021 Jun 24];50:67-80. Available from: https://www.scielo.br/j/rbr/a/5BcvSsQGhJPXXD8Q9Pzff8H/?lang=en#
McCullough PJ, Lehrer DS, Amend J. Daily oral dosing of vitamin D3 using 5000 TO 50,000 international units a day in long-term hospitalized patients: Insights from a seven year experience. The Journal of Steroid Biochemistry and Molecular Biology [Internet]. 2019 May 1 [cited 2021 Jun 25];189:228-39. Available from: https://www.sciencedirect.com/science/article/pii/S0960076018306228
Kagotho E, Omuse G, Okinda N, Ojwang P. Vitamin D status in healthy black African adults at a tertiary hospital in Nairobi, Kenya: a cross sectional study. BMC Endocr Disord [Internet]. 2018 Oct 11 [cited 2021 Jun 30];18:70. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6180659/
Luxwolda MF, Kuipers RS, Kema IP, van der Veer E, Dijck-Brouwer DAJ, Muskiet FAJ. Vitamin D status indicators in indigenous populations in East Africa. Eur J Nutr. 2013 Apr;52(3):1115-25.
Holick MF. VITAMIN D STATUS: MEASUREMENT, INTERPRETATION AND CLINICAL APPLICATION. Ann Epidemiol [Internet]. 2009 Feb [cited 2020 May 23];19(2):73-8. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2665033/
Kaufman HW, Niles JK, Kroll MH, Bi C, Holick MF. SARS-CoV-2 positivity rates associated with circulating 25-hydroxyvitamin D levels. PLOS ONE [Internet]. 2020 Sep 17 [cited 2020 Dec 8];15(9):e0239252. Available from: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0239252
Christakos S, Li S, De La Cruz J, Bikle DD. New developments in our understanding of vitamin D metabolism, action and treatment. Metabolism [Internet]. 2019 Sep 1 [cited 2020 Jun 5];98:112-20. Available from: http://www.sciencedirect.com/science/article/pii/S0026049519301192
Jovic TH, Ali SR, Ibrahim N, Jessop ZM, Tarassoli SP, Dobbs TD, et al. Could Vitamins Help in the Fight Against COVID-19? Nutrients [Internet]. 2020 Sep [cited 2020 Dec 2];12(9):2550. Available from: https://www.mdpi.com/2072-6643/12/9/2550
Veugelers P, Ekwaru J. A Statistical Error in the Estimation of the Recommended Dietary Allowance for Vitamin D. Nutrients [Internet]. 2014 Oct 20 [cited 2020 Jun 17];6(10):4472-5. Available from: http://www.mdpi.eom/2072-6643/6/10/4472
Heaney R, Garland C, Baggerly C, French C, Gorham E. Letter to Veugelers, P.J. and Ekwaru, J.P., A statistical error in the estimation of the recommended dietary allowance for vitamin D. Nutrients 2014, 6, 4472-4475; doi:10.3390/nu6104472. Nutrients. 2015 Mar 10;7(3):1688-90.
Grassroots Health. GrassrootsHealth Data supports much higher vitamin D RDA [Internet]. GrassrootsHealth. 2015 [cited 2021 Jun 28]. Available from:https://www.grassrootshealth.net/blog/grassrootshealth-data-supports-much-higher-intake-of-vitamin-d-than-the-current-rda/
Bleizgys A. Vitamin D and COVID-19: It is time to act. International Journal of Clinical Practice [Internet]. 2021 [cited 2021 Jun 24];75(3):e13748. Available from: https://onlinelibrary.wiley.com/doi/abs/10.1111/ijcp.13748
Grant WB, Lahore H, McDonnell SL, Baggerly CA, French CB, Aliano JL, et al. Evidence that Vitamin D Supplementation Could Reduce Risk of Influenza and COVID-19 Infections and Deaths. Nutrients [Internet]. 2020 Apr [cited 2020 Jun 22];12(4):988. Available from: https://www.mdpi.com/2072- 6643/12/4/988
Grant WB, McDonnell SL. Letter in response to the article: Vitamin D concentrations and COVID-19 infection in UK biobank (Hastie et al.). Diabetes & Metabolic Syndrome: Clinical Research & Reviews [Internet]. 2020 Sep 1 [cited 2020 Jun 22];14(5):893-4. Available from: http://www.sciencedirect.com/science/article/pii/S1871402120301648
Afshar P, Ghaffaripour M, Sajjadi H. Suggested role of Vitamin D supplementation in COVID-19 severity. Journal of Contemporary Medical Sciences [Internet]. 2020 Aug 26 [cited 2020 Dec 2];6(4). Available from: http://www.jocms.org/index.php/jcms/article/view/822
Holick MF. The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Rev Endocr Metab Disord. 2017;18(2):153-65.
van Schoor N, Lips P. Global Overview of Vitamin D Status. Endocrinology and Metabolism Clinics of North America [Internet]. 2017 Dec 1 [cited 2020 Dec 14];46(4):845-70. Available from: http://www.sciencedirect.com/science/article/pii/S0889852917300646
National Institutes of Health. Vitamin D [Internet]. COVID-19 Treatment Guidelines. [cited 2021 Jun 24]. Available from: https://www.covid19treatmentguidelines.nih.gov/therapies/supplements/vitamin-d/
Coronavirus disease - Answers [Internet]. [cited 2021 Jun 24]. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/coronavirus-disease-answers
BDA. COVID-19 / Coronavirus - Advice for the General Public [Internet]. [cited 2021 Jun 24]. Available from: https://www.bda.uk.com/resource/covid-19-corona-virus-advice-for-the-general-public.html
Vitamins and minerals - Vitamin D [Internet]. nhs.uk. 2017 [cited 2020 May 20]. Available from: https://www.nhs.uk/conditions/vitamins-and-minerals/vitamin-d/
Marcinowska-Suchowierska E, Kupisz-Urbanska M, Lukaszkiewicz J, Pludowski P, Jones G. Vitamin D Toxicity-A Clinical Perspective. Front Endocrinol [Internet]. 2018 [cited 2020 Jun 23];9. Available from: https://www.frontiersin.org/articles/10.3389/fendo.2018.00550/full
Taylor PN, Davies JS. A review of the growing risk of vitamin D toxicity from inappropriate practice. Br J Clin Pharmacol [Internet]. 2018 Jun [cited 2021 Jun 26];84(6):1121-7. Available from: https://www.ncbi.nIm.nih.gov/pmc/artides/PMC5980613/
Asif A, Farooq N. Vitamin D Toxicity. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 [cited 2021 Jun 26]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK557876/
Araki T, Holick MF, Alfonso BD, Charlap E, Romero CM, Rizk D, et al. Vitamin D Intoxication with Severe Hypercalcemia due to Manufacturing and Labeling Errors of Two Dietary Supplements Made in the United States. The Journal of Clinical Endocrinology & Metabolism [Internet]. 2011 Dec 1 [cited 2021 Aug 20];96(12):3603-8. Available from: https://doi.org/10.1210/jc.2011-1443
Saul AW. Vitamin D: Deficiency, Diversity and Dosage. JOM [Internet]. 2003 [cited 2021 Jun 28];18(3- 4):194-204. Available from: https://isom.ca/jom-archives/vol18-no3-4-2003/
Stipp D. Vitamin D Level in Milk, Infant Formula Is Often Too High or Low, Survey Says. Wall Street Journal. Eastern Edition. 1992 Apr 30;6.
Norfolk County Ct 380. TARPEY vs. CRESCENT RIDGE DAIRY, INC., 47 Mass. App. Ct. 380 [Internet]. 1999 [cited 2021 Jun 28]. Available from: http://masscases.com/cases/app/47/47massappct380.html
Shirvani A, Kalajian TA, Song A, Holick MF. Disassociation of Vitamin D’s Calcemic Activity and Non- calcemic Genomic Activity and Individual Responsiveness: A Randomized Controlled Double-Blind Clinical Trial. Sci Rep [Internet]. 2019 Nov 27 [cited 2021 Aug 20];9(1):17685. Available from: https://www.nature.com/articles/s41598-019-53864-1
Martineau AR, Jolliffe DA, Hooper RL, Greenberg L, Aloia JF, Bergman P, et al. Vitamin D supplementation to prevent acute respiratory tract infections: systematic review and meta-analysis of individual participant data. BMJ [Internet]. 2017 Feb 15 [cited 2020 May 8];356. Available from: https ://www.bmj .com/content/356/bmj .i6583
Kimball SM, Mirhosseini N, Holick MF. Evaluation of vitamin D3 intakes up to 15,000 international units/day and serum 25-hydroxyvitamin D concentrations up to 300 nmol/L on calcium metabolism in a community setting. Dermatoendocrinol [Internet]. 2017 Apr 13 [cited 2020 Jun 20];9(1). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5402701/
Jolliffe DA, Camargo CA, Sluyter JD, Aglipay M, Aloia JF, Ganmaa D, et al. Vitamin D supplementation to prevent acute respiratory infections: a systematic review and meta-analysis of aggregate data from randomised controlled trials. The Lancet Diabetes & Endocrinology [Internet]. 2021 May 1 [cited 2021 Apr 24];9(5):276-92. Available from: https://www.thelancet.com/journals/landia/article/PIIS2213- 8587(21)00051-6/abstract
Lakkireddy M, Gadiga SG, Malathi RD, Karra ML, Raju ISSVPM, Ragini, et al. Impact of daily high dose oral vitamin D therapy on the inflammatory markers in patients with COVID 19 disease. Scientific Reports [Internet]. 2021 May 20 [cited 2021 May 21];11(1):10641. Available from:https ://www. nature.com/articles/s41598-021-90189-4
Rastogi A, Bhansali A, Khare N, Suri V, Yaddanapudi N, Sachdeva N, et al. Short term, high-dose vitamin D supplementation for COVID-19 disease: a randomised, placebo-controlled, study (SHADE study). Postgraduate Medical Journal [Internet]. 2020 Nov 12 [cited 2020 Dec 14]; Available from: https://pmj.bmj.com/content/early/2020/11/12/postgradmedj-2020-139065
Annweiler C, Hanotte B, de l’Eprevier CG, Sabatier J-M, Lafaie L, Celarier T. Vitamin D and survival in COVID-19 patients: A quasi-experimental study. The Journal of Steroid Biochemistry and Molecular
Biology [Internet]. 2020 Oct 13 [cited 2020 Oct 19];105771. Available from: http://www.sciencedirect.com/science/article/pii/S096007602030296X
Srivastava A, Gupta RC, Doss RB, Lall R. Trace Minerals, Vitamins and Nutraceuticals in Prevention and Treatment of COVID-19. Journal of Dietary Supplements [Internet]. 2021 [cited 2021 Apr 4] ;1 —3 5. Available from: https://app.dimensions.ai/details/publication/pub. 1136165220
Aranow C. Vitamin D and the Immune System. Journal of Investigative Medicine [Internet]. 2011 Aug 1 [cited 2020 May 4];59(6):881-6. Available from: https://jim.bmj.com/content/59/6/881
Corrao S, Mallaci Bocchio R, Lo Monaco M, Natoli G, Cavezzi A, Troiani E, et al. Does Evidence Exist to Blunt Inflammatory Response by Nutraceutical Supplementation during COVID-19 Pandemic? An Overview of Systematic Reviews of Vitamin D, Vitamin C, Melatonin, and Zinc. Nutrients. 2021 Apr 12;13(4).
Mercola J, Grant WB, Wagner CL. Evidence Regarding Vitamin D and Risk of COVID-19 and Its Severity. Nutrients [Internet]. 2020 Nov [cited 2020 Dec 24];12(11):3361. Available from: https://www.mdpi.com/2072-6643/12/11/3361
Cavezzi A, Troiani E, Corrao S. COVID-19: Hemoglobin, Iron, and Hypoxia beyond Inflammation. A Narrative Review. Clinics and Practice [Internet]. 2020 May [cited 2021 Jun 25];10(2):24-30. Available from: https://www.mdpi.com/2039-7283/10/2/1271
Boucher BJ. The Problems of Vitamin D Insufficiency in Older People. Aging Dis [Internet]. 2012 Jun 6 [cited 2020 Apr 23];3(4):313-29. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3501367/
Sabetta JR, DePetrillo P, Cipriani RJ, Smardin J, Burns LA, Landry ML. Serum 25-Hydroxyvitamin D and the Incidence of Acute Viral Respiratory Tract Infections in Healthy Adults. PLoS One [Internet]. 2010 Jun 14 [cited 2020 Apr 23];5(6). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2885414/
Ahmed A, Siman-Tov G, Hall G, Bhalla N, Narayanan A. Human Antimicrobial Peptides as Therapeutics for Viral Infections. Viruses [Internet]. 2019 Aug 1 [cited 2021 Jun 25];11(8):704. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6722670/
Martinez-Moreno J, Hernandez JC, Urcuqui-Inchima S. Effect of high doses of vitamin D supplementation on dengue virus replication, Toll-like receptor expression, and cytokine profiles on dendritic cells. Mol Cell Biochem. 2020 Jan;464(1-2):169-80.
King EM. T-cells really are the superstars in fighting COVID-19 - but why are some of us so poor at making them? BMJ (British Medical Journal) [Internet]. 2021 Jun 14 [cited 2021 Jun 25];2020(370):m3563/rr-6. Available from: https://www.bmj.com/content/370/bmj.m3563/rr-6
Sekine T, Perez-Potti A, Rivera-Ballesteros O, Stralin K, Gorin J-B, Olsson A, et al. Robust T Cell Immunity in Convalescent Individuals with Asymptomatic or Mild COVID-19. Cell [Internet]. 2020 Oct 1 [cited 2020 Oct 30];183(1):158-168.e14. Available from: http://www.sciencedirect.com/science/article/pii/S0092867420310084
Mohd S, Sharma S, Mishra A, Ashraf MZ. Vitamin D and Its Relationship with the Pathways Related to Thrombosis and Various Diseases [Internet]. IntechOpen; 2021 [cited 2021 May 19]. Available from: https://www.intechopen.com/online-first/vitamin-d-and-its-relationship-with-the-pathways-related-to- thrombosis-and-various-diseases
Jain A, Chaurasia R, Sengar NS, Singh M, Mahor S, Narain S. Analysis of vitamin D level among asymptomatic and critically ill COVID-19 patients and its correlation with inflammatory markers. Sci Rep [Internet]. 2020 Nov 19 [cited 2021 Jun 26];10(1):20191. Available from: https://www.nature.com/artides/s41598-020-77093-z
Timms PM, Mannan N, Hitman GA, Noonan K, Mills PG, Syndercombe-Court D, et al. Circulating MMP9, vitamin D and variation in the TIMP-1 response with VDR genotype: mechanisms for inflammatory damage in chronic disorders? QJM. 2002 Dec;95(12):787-96.
Rabaan AA, Al-Ahmed SH, Garout MA, Al-Qaaneh AM, Sule AA, Tirupathi R, et al. Diverse Immunological Factors Influencing Pathogenesis in Patients with COVID-19: A Review on Viral Dissemination, Immunotherapeutic Options to Counter Cytokine Storm and Inflammatory Responses. Pathogens [Internet]. 2021 May [cited 2021 May 10];10(5):565. Available from: https://www.mdpi.com/2076-0817/10/5/565
Price LC, McCabe C, Garfield B, Wort SJ. Thrombosis and COVID-19 pneumonia: the clot thickens! European Respiratory Journal [Internet]. 2020 Jul 1 [cited 2021 Jun 26];56(1). Available from: https://erj.ersjournals.com/content/56/1/2001608
Connors JM, Levy JH. COVID-19 and its implications for thrombosis and anticoagulation. Blood [Internet]. 2020 Jun 4 [cited 2021 Jun 26];135(23):2033-40. Available from:https://doi.org/10.1182/blood.2020006000
Chambers ES, Vukmanovic-Stejic M, Turner CT, Shih BB, Trahair H, Pollara G, et al. Vitamin D3 replacement enhances antigen-specific immunity in older adults. Immunotherapy Advances [Internet]. 2020 Nov 25 [cited 2020 Dec 21];(ltaa008). Available from: https://doi.org/10.1093/immadv/ltaa008
Brown RA, Sarkar A. Vitamin D deficiency: a factor in COVID-19, progression, severity and mortality? - An urgent call for research. MitoFit Preprint Arch [Internet]. 2020 Feb 29 [cited 2021 Jun 27]; Available from: https://www.mitofit.org/index.php/Brown2020MitoFitPreprintArch
BAPIO and BMA raise concerns over ethnic minority doctor deaths to Covid-19 [Internet]. Pulse Today. 2020 [cited 2021 Jun 27]. Available from: https://www.pulsetoday.co.uk/news/uncategorised/bapio-and- bma-raise-concerns-over-ethnic-minority-doctor-deaths-to-covid-19/
Cook T, Kursumovic E, Lennane S. Exclusive: deaths of NHS staff from covid-19 analysed [Internet]. Health Service Journal. 2020 [cited 2020 Jun 24]. Available from: https://www.hsj.co.uk/exclusive-deaths- of-nhs-staff-from-covid-19-analysed/7027471.article
Grimes DS. Covid-19 & Vitamin D : Deaths of doctors from Covid-19 [Internet]. Dr David Grimes, Consultant physician and gastroenterologist. 2020 [cited 2021 Jun 27]. Available from: http://www.drdavidgrimes.com/2020/11/covid-19-vitamin-d-deaths-of-doctors.html
Grimes DS. Covid-19 & Vitamin D: There is no African Paradox [Internet]. Dr David Grimes, Consultant physician and gastroenterologist. 2021 [cited 2021 Jun 27]. Available from: http://www.drdavidgrimes.com/2021/04/covid-19-vitamin-d-there-is-no-african.html
Grimes DS. Covid-19 & Vitamin D : The common link. Remember William of Ockham? [Internet]. Dr David Grimes, Consultant physician and gastroenterologist. 2021 [cited 2021 Jun 27]. Available from: http://www.drdavidgrimes.com/2021/02/covid-19-vitamin-d-disappearance-of.html
Cannell JJ, Vieth R, Umhau J, Holick MF, Grant WB, Madronich S, et al. Epidemic influenza and vitamin D. Epidemiol Infect [Internet]. 2006 Dec [cited 2020 May 8];134(6):1129-40. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2870528/
Roth DE, Abrams SA, Aloia J, Bergeron G, Bourassa MW, Brown KH, et al. Global prevalence and disease burden of vitamin D deficiency: a roadmap for action in low- and middle-income countries. Ann N Y Acad
Sci [Internet]. 2018 Oct [cited 2021 Jun 10];1430(1):44-79. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7309365/
Pfleger K, Davies G, Boucher BJ, Umhau J, Kimball SM, Thakkar V, et al. Over 200 Scientists, Doctors, & Leading Authorities Call For Increased Vitamin D Use To Combat COVID-19 [Internet]. Vitamin D For All Collaboration; 2020. Available from: https://vitamindforall.org/letter.html
Pugach IZ, Pugach S. Strong correlation between prevalence of severe vitamin D deficiency and population mortality rate from COVID-19 in Europe. Wien Klin Wochenschr [Internet]. 2021 Mar 15 [cited 2021 Jun 27];1-3. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7957444/
Walrand S. Autumn COVID-19 surge dates in Europe correlated to latitudes, not to temperature-humidity, pointing to vitamin D as contributing factor. Sci Rep [Internet]. 2021 Jan 21 [cited 2021 Jul 22];11(1):1981. Available from: https://www.nature.com/articles/s41598-021-81419-w
Worldometer. Coronavirus Graphs: Worldwide Cases and Deaths - Worldometer [Internet]. covid-19 CORONAVIRUS. 2021 [cited 2021 Jun 27]. Available from: https://www.worldometers.info/coronavirus/worldwide-graphs/#countries-cases
Isaia G, Diémoz H, Maluta F, Fountoulakis I, Ceccon D, di Sarra A, et al. Does solar ultraviolet radiation play a role in COVID-19 infection and deaths? An environmental ecological study in Italy. Science of The Total Environment [Internet]. 2021 Feb 25 [cited 2021 Jun 27];757:143757. Available from: https://www.sciencedirect.com/science/article/pii/S0048969720372880
Jayawardena R, Jeyakumar DT, Francis TV, Misra A. Impact of the vitamin D deficiency on COVID-19 infection and mortality in Asian countries. Diabetes & Metabolic Syndrome: Clinical Research & Reviews [Internet]. 2021 May [cited 2021 Apr 7];15(3):757-64. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1871402121000746
Herrera-Quintana L, Gamarra-Morales Y, Vázquez-Lorente H, Molina-López J, Castaño-Pérez J, Machado- Casas JF, et al. Bad Prognosis in Critical Ill Patients with COVID-19 during Short-Term ICU Stay regarding Vitamin D Levels. Nutrients [Internet]. 2021 Jun [cited 2021 Jun 18];13(6):1988. Available from: https://www.mdpi.com/2072-6643/13/6/1988
Merzon E, Tworowski D, Gorohovski A, Vinker S, Cohen AG, Green I, et al. Low plasma 25(OH) vitamin D level is associated with increased risk of COVID-19 infection: an Israeli population-based study. The FEBS Journal [Internet]. 2020 [cited 2020 Oct 25];287(17):3693-702. Available from: https://febs.onlinelibrary.wiley.com/doi/abs/10.1111/febs. 15495
Meltzer DO, Best TJ, Zhang H, Vokes T, Arora VM, Solway J. Association of Vitamin D Levels, Race/Ethnicity, and Clinical Characteristics With COVID-19 Test Results. JAMA Network Open [Internet]. 2021 Mar 19 [cited 2021 Apr 4];4(3):e214117-e214117. Available from:https://doi.org/10.1001/jamanetworkopen.2021.4117
Katz J, Yue S, Xue W. Increased risk for COVID-19 in patients with vitamin D deficiency. Nutrition [Internet]. 2021 Apr 1 [cited 2021 Jan 8];84:111106. Available from: http://www.sciencedirect.com/science/article/pii/S0899900720303890
Liu N, Sun J, Wang X, Zhang T, Zhao M, Li H. Low vitamin D status is associated with coronavirus disease 2019 outcomes: a systematic review and meta-analysis. International Journal of Infectious Diseases [Internet]. 2021 Mar 1 [cited 2021 Jun 28];104:58-64. Available from: https://www.ijidonline.com/article/S1201 -9712(20)32600-X/abstract
Nikniaz L, Akbarzadeh MA, Hosseinifard H, Hosseini M-S. The impact of vitamin D supplementation on mortality rate and clinical outcomes of COVID-19 patients: A systematic review and meta-analysis.
medRxiv [Internet]. 2021 Jan 5 [cited 2021 Jan 8];2021.01.04.21249219. Available from: https://www.medrxiv.org/content/10.1101/2021.01.04.21249219v1
Carpagnano GE, Di Lecce V, Quaranta VN, Zito A, Buonamico E, Capozza E, et al. Vitamin D deficiency as a predictor of poor prognosis in patients with acute respiratory failure due to COVID-19. J Endocrinol Invest [Internet]. 2020 Aug 9 [cited 2020 Nov 24];1-7. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7415009/
Szarpak L, Rafique Z, Gasecka A, Chirico F, Gawel W, Hernik J, et al. A systematic review and metaanalysis of effect of vitamin D levels on the incidence of COVID-19. Cardiol J. 2021 Jul 26;
Ghasemian R, Shamshirian A, Heydari K, Malekan M, Alizadeh-Navaei R, Ebrahimzadeh MA, et al. The role of vitamin D in the age of COVID-19: A systematic review and meta-analysis. International Journal of Clinical Practice [Internet]. 2021 [cited 2021 Aug 20];n/a(n/a):e14675. Available from: https://onlinelibrary.wiley.com/doi/abs/10.1111/ijcp. 14675
Lappe JM, Heaney RP. Why randomized controlled trials of calcium and vitamin D sometimes fail. Dermatoendocrinol [Internet]. 2012 Apr 1 [cited 2021 Jun 29];4(2):95-100. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3427206/
Griffin G, Hewison M, Hopkin J, Kenny R, Quinton R, Rhodes J, et al. Vitamin D and COVID-19: evidence and recommendations for supplementation. Royal Society Open Science [Internet]. 2020 [cited 2021 Jun 29];7(12):201912. Available from: https://royalsocietypublishing.org/doi/10.1098/rsos.201912
Annweiler C, Cao Z, Sabatier J-M. Point of view: Should COVID-19 patients be supplemented with vitamin D? Maturitas [Internet]. 2020 Oct [cited 2020 Jun 18];140:24-6. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0378512220302929
Davies G, Garami AR, Byers JC. Evidence Supports a Causal Role for Vitamin D Status in COVID-19 Outcomes. medRxiv [Internet]. 2020 Jun 13 [cited 2020 Jun 16];2020.05.01.20087965. Available from: https://www.medrxiv.org/content/10.1101/2020.05.01.20087965v3
Boucher BJ. Why do so many trials of vitamin D supplementation fail? Endocr Connect [Internet]. 2020 Aug 11 [cited 2021 Jun 29];9(9):R195-206. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7487184/
Grant WB, Boucher BJ, Bhattoa HP, Lahore H. Why vitamin D clinical trials should be based on 25- hydroxyvitamin D concentrations. The Journal of Steroid Biochemistry and Molecular Biology [Internet]. 2018 Mar 1 [cited 2021 Jun 29];177:266-9. Available from: https://www.sciencedirect.com/science/article/pii/S0960076017302236
Griffin G, Hewison M, Hopkin J, Kenny RA, Quinton R, Rhodes J, et al. Perspective: Vitamin D supplementation prevents rickets and acute respiratory infections when given as daily maintenance but not as intermittent bolus: implications for COVID-19. Clin Med (Lond) [Internet]. 2021 Mar [cited 2021 Jun 12];21(2):e144-9. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8002781/
Davies G, Mazess R, Benskin LL. Letter to the editor in response to the article: “Vitamin D concentrations and COVID-19 infection in UK Biobank” (Hastie et al). Diabetes & Metabolic Syndrome: Clinical Research & Reviews [Internet]. 2021 Feb 9 [cited 2021 Feb 10]; Available from: https://www.sciencedirect.com/science/article/pii/S1871402121000394
Annweiler G, Corvaisier M, Gautier J, Dubee V, Legrand E, Sacco G, et al. Vitamin D Supplementation Associated to Better Survival in Hospitalized Frail Elderly COVID-19 Patients: The GERiA-COVID QuasiExperimental Study. Nutrients [Internet]. 2020 Nov [cited 2021 Feb 2];12(11):3377. Available from: https://www.mdpi.com/2072-6643/12/11/3377
Cangiano B, Fatti LM, Danesi L, Gazzano G, Croci M, Vitale G, et al. Mortality in an Italian nursing home during COVID-19 pandemic: correlation with gender, age, ADL, vitamin D supplementation, and limitations of the diagnostic tests. Aging (Albany NY). 2020 Dec 22;12(24):24522-34.
Hernández JL, Nan D, Fernandez-Ayala M, García-Unzueta M, Hernández-Hernández MA, López-Hoyos M, et al. Vitamin D Status in Hospitalized Patients with SARS-CoV-2 Infection. J Clin Endocrinol Metab. 2021 Mar 8;106(3):e1343-53.
Oristrell J, Oliva JC, Subirana I, Casado E, Dominguez D, Toloba A, et al. Association of Calcitriol Supplementation with Reduced COVID-19 Mortality in Patients with Chronic Kidney Disease: A Population-based Study. 2021 Apr 6 [cited 2021 Apr 12]; Available from: https://www.preprints.org/manuscript/202104.0173/v1
Fasano A, Cereda E, Barichella M, Cassani E, Ferri V, Zecchinelli AL, et al. COVID-19 in Parkinson’s Disease Patients Living in Lombardy, Italy. Mov Disord. 2020 Jul;35(7):1089-93.
Israel A, Cicurel AA, Feldhamer I, Dror Y, Giveon SM, Gillis D, et al. The link between vitamin D deficiency and Covid-19 in a large population. medRxiv [Internet]. 2020 Sep 7 [cited 2020 Nov 24];2020.09.04.20188268. Available from:
https://www.medrxiv.org/content/10.1101/2020.09.04.20188268v1
Ma H, Zhou T, Heianza Y, Qi L. Habitual use of vitamin D supplements and risk of coronavirus disease 2019 (COVID-19) infection: a prospective study in UK Biobank. Am J Clin Nutr. 2021 May 8;113(5):1275- 81.
Loucera C, Peña-Chilet M, Esteban-Medina M, Muñoyerro-Muñiz D, Villegas R, Lopez-Miranda J, et al. Real world evidence of calcifediol use and mortality rate of COVID-19 hospitalized in a large cohort of 16,401 Andalusian patients. medRxiv [Internet]. 2021 Apr 29 [cited 2021 Jun 25];2021.04.27.21255937. Available from: https://www.medrxiv.org/content/10.1101/2021.04.27.21255937v1
Murai IH, Fernandes AL, Sales LP, Pinto AJ, Goessler KF, Duran CSC, et al. Effect of Vitamin D3 Supplementation vs Placebo on Hospital Length of Stay in Patients with Severe COVID-19: A Multicenter, Double-blind, Randomized Controlled Trial. medRxiv [Internet]. 2020 Nov 17 [cited 2020 Nov 18];2020.11.16.20232397. Available from: https://www.medrxiv.org/content/10.1101/2020.11.16.20232397v1
Jevalikar G, Mithal A, Singh A, Sharma R, Farooqui KJ, Mahendru S, et al. Lack of association of baseline 25-hydroxyvitamin D levels with disease severity and mortality in Indian patients hospitalized for COVID- 19. Scientific Reports [Internet]. 2021 Mar 18;11(1):6258. Available from: https://doi.org/10.1038/s41598- 021-85809-y
Ling SF, Broad E, Murphy R, Pappachan JM, Pardesi-Newton S, Kong M-F, et al. High-Dose Cholecalciferol Booster Therapy is Associated with a Reduced Risk of Mortality in Patients with COVID- 19: A Cross-Sectional Multi-Centre Observational Study. Nutrients [Internet]. 2020 Dec [cited 2020 Dec 12];12(12):3799. Available from: https://www.mdpi.com/2072-6643/12/12/3799
Giannini S, Passeri G, Tripepi G, Sella S, Fusaro M, Arcidiacono G, et al. Effectiveness of In-Hospital Cholecalciferol Use on Clinical Outcomes in Comorbid COVID-19 Patients: A Hypothesis-Generating Study. Nutrients [Internet]. 2021 Jan [cited 2021 Jan 19];13(1):219. Available from: https://www.mdpi.com/2072-6643/13/1/219
Ohaegbulam KC, Swalih M, Patel P, Smith MA, Perrin R. Vitamin D Supplementation in COVID-19 Patients: A Clinical Case Series. American Journal of Therapeutics [Internet]. 2020 Oct [cited 2020 Dec 3];27(5):e485. Available from: https://joumals.lww.com/americantherapeutics/Abstract/2020/10000/VitaminDSupplementationinCOV ID_ 19_Patients A. 8.aspx
Sabico S, Enani MA, Sheshah E, Aljohani NJ, Aldisi DA, Alotaibi NH, et al. Effects of a 2-Week 5000 IU versus 1000 IU Vitamin D3 Supplementation on Recovery of Symptoms in Patients with Mild to Moderate Covid-19: A Randomized Clinical Trial. Nutrients [Internet]. 2021 Jul [cited 2021 Jun 28];13(7):2170. Available from: https://www.mdpi.com/2072-6643/13/7/2170
Tan CW, Ho LP, Kalimuddin S, Cherng BPZ, Teh YE, Thien SY, et al. Cohort study to evaluate the effect of vitamin D, magnesium, and vitamin B12 in combination on progression to severe outcomes in older patients with coronavirus (COVID-19). Nutrition. 2020 Dec;79-80:111017.
Entrenas Castillo M, Entrenas Costa LM, Vaquero Barrios JM, Alcalá Díaz JF, López Miranda J, Bouillon R, et al. “Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot randomized clinical study.” J Steroid Biochem Mol Biol [Internet]. 2020 Oct [cited 2020 Sep 22] ;203:105751. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7456194/
Alcala-Diaz JF, Limia-Perez L, Gomez-Huelgas R, Martin-Escalante MD, Cortes-Rodriguez B, Zambrana- Garcia JL, et al. Calcifediol Treatment and Hospital Mortality Due to COVID-19: A Cohort Study. Nutrients [Internet]. 2021 Jun [cited 2021 Jun 2];13(6):1760. Available from: https://www.mdpi.com/2072- 6643/13/6/1760
Nogués X, Ovejero D, Quesada-Gomez JM, Bouillon R, Arenas D, Pascual J, et al. Calcifediol Treatment and COVID-19-Related Outcomes [Internet]. Rochester, NY: Social Science Research Network; 2021 Jan [cited 2021 Feb 12]. Report No.: ID 3771318. Available from: https://papers.ssrn.com/abstract=3771318
Quesada-Gomez JM, Bouillon R. Is calcifediol better than cholecalciferol for vitamin D supplementation? Osteoporos Int. 2018 Aug;29(8):1697-711.
Vitamina D nella prevenzione e nel trattamento del COVID-19: nuove evidenze (3 dicembre 2020)
[Internet]. [cited 2021 Sep 5]. Available from: https://www.accademiadimedicina.unito.it/attivita/altro/317- vitamina-d-nella-prevenzione-e-nel-trattamento-del-covid-19-nuove-evidenze.html
Effet bénéfique de la vitamine D dans la Covid : quelles sont les données ? [Internet]. [cited 2021 Sep 5]. Available from: https://www.larevuedupraticien.fr/article/effet-benefique-de-la-vitamine-d-dans-la-covid- quelles-sont-les-donnees
McCartney DM, O’Shea PM, Faul JL, Healy MJ, Byrne G, Griffin TP, et al. Vitamin D and SARS-CoV-2 infection—evolution of evidence supporting clinical practice and policy development. Ir J Med Sci [Internet]. 2020 Nov 21 [cited 2020 Dec 2]; Available from: https://doi.org/10.1007/s11845-020-02427-9
Oireachtas H of the. Oireachtas Health Committee launches report on addressing Vitamin D deficiency in Ireland - 7 Apr 2021, 11.00 - Houses of the Oireachtas [Internet]. 2021 [cited 2021 Sep 5]. Available from: https://www.oireachtas.ie/en/press-centre/press-releases/20210407-oireachtas-health-committee-launches- report-on-addressing-vitamin-d-deficiency-in-ireland
Akbar MR, Wibowo A, Pranata R, Setiabudiawan B. Low Serum 25-hydroxyvitamin D (Vitamin D) Level Is Associated With Susceptibility to COVID-19, Severity, and Mortality: A Systematic Review and MetaAnalysis. Front Nutr [Internet]. 2021 [cited 2021 Jun 26];8. Available from: https://www.frontiersin.org/articles/10.3389/fnut.2021.660420/full
Artusi CA, Romagnolo A, Ledda C, Zibetti M, Rizzone MG, Montanaro E, et al. COVID-19 and Parkinson’s Disease: What Do We Know So Far? J Parkinsons Dis [Internet]. 2021 [cited 2021 Jun 10];11(2):445-54. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8150504/
Bassatne A, Basbous M, Chakhtoura M, El Zein O, Rahme M, El-Hajj Fuleihan G. The link between COVID-19 and Vitamin D (VIVID): A systematic review and meta-analysis. Metabolism [Internet]. 2021 Jun [cited 2021 Jul 1];119:154753. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0026049521000536
Chambergo-Michilot D, Barros-Sevillano S, Rivera-Torrejon O, De la Cruz-Ku GA, Custodio N. Factors associated with COVID-19 in people with Parkinson’s disease: a systematic review and meta-analysis. Eur J Neurol. 2021 May 13;
Chen J, Xie L, Yuan P, Ma J, Yu P, Zheng C, et al. Low serum vitamin D level and COVID-19 infection and outcomes, a multivariate meta-analysi [Internet]. 2020 [cited 2021 Jun 26]. Available from: https://europepmc.org/article/PPR/PPR230641
Damayanthi HDWT, Prabani KIP. Nutritional determinants and COVID-19 outcomes of older patients with COVID-19: A systematic review. Arch Gerontol Geriatr. 2021 Aug;95:104411.
Das P, Samad N, Ahinkorah BO, Peprah P, Mohammed A, Seidu A-A. Effect of Vitamin D deficiency on COVID-19 status: A systematic review. medRxiv [Internet]. 2020 Dec 3 [cited 2020 Dec 14];2020.12.01.20242313. Available from: https://www.medrxiv.org/content/10.1101/2020.12.01.20242313v1
Drame M, Cofais C, Hentzien M, Proye E, Coulibaly PS, Demoustier-Tampere D, et al. Relation between Vitamin D and COVID-19 in Aged People: A Systematic Review. Nutrients [Internet]. 2021 Apr [cited 2021 May 18];13(4):1339. Available from: https://www.mdpi.com/2072-6643/13/4Z1339
Grove A, Osokogu O, Al-Khudairy L, Mehrabian A, Zanganeh M, Brown A, et al. Association between vitamin D supplementation or serum vitamin D level and susceptibility to SARS-CoV-2 infection or COVID-19 including clinical course, morbidity and mortality outcomes? A systematic review. BMJ Open. 2021 May 28;11(5):e043737.
Munshi R, Hussein MH, Toraih EA, Elshazli RM, Jardak C, Sultana N, et al. Vitamin D insufficiency as a potential culprit in critical COVID-19 patients. J Med Virol. 2020 Jul 27;93(2):733-40.
Pereira M, Damascena AD, Azevedo LMG, Oliveira T de A, Santana J da M. Vitamin D deficiency aggravates COVID-19: systematic review and meta-analysis. Critical Reviews in Food Science and Nutrition [Internet]. 2020 Nov 4 [cited 2020 Nov 5];0(0):1-9. Available from: https://doi.org/10.1080/10408398.2020.1841090
Petrelli F, Luciani A, Perego G, Dognini G, Colombelli PL, Ghidini A. Therapeutic and prognostic role of vitamin D for COVID-19 infection: A systematic review and meta-analysis of 43 observational studies. J Steroid Biochem Mol Biol [Internet]. 2021 Jul [cited 2021 Jun 10];211:105883. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7997262/
Rothenberg E. Coronavirus Disease 19 from the Perspective of Ageing with Focus on Nutritional Status and Nutrition Management—A Narrative Review. Nutrients [Internet]. 2021 Apr [cited 2021 Apr 24];13(4):1294. Available from: https://www.mdpi.com/2072-6643/13/4/1294
Shah K, Saxena D, Mavalankar D. Vitamin D supplementation, COVID-19 and disease severity: a metaanalysis. QJM. 2021 May 19;114(3):175-81.
Stroehlein JK, Wallqvist J, Iannizzi C, Mikolajewska A, Metzendorf M-I, Benstoem C, et al. Vitamin D supplementation for the treatment of COVID-19: a living systematic review. Cochrane Database Syst Rev. 2021 May 24;5:CD015043.
Teshome A, Adane A, Girma B, Mekonnen ZA. The Impact of Vitamin D Level on COVID-19 Infection: Systematic Review and Meta-Analysis. Front Public Health [Internet]. 2021 Mar 5 [cited 2021 Jun 10];9. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7973108/
Wang Z, Joshi A, Leopold K, Jackson S, Christensen S, Nayfeh T, et al. Association of Vitamin D Deficiency with COVID-19 Infection Severity: Systematic Review and Meta-analysis. Clin Endocrinol (Oxf). 2021 Jun 23;
Yadav SK, Gaurav K, Johri G, Jaiswal SK, Jha CK, Yadav N. A systematic review of the role of hypovitaminosis D in coronavirus disease-19 (COVID-19) infection and mortality: Is there a role of recommending high dose vitamin D supplementation? Human Nutrition & Metabolism [Internet]. 2021 Mar 1 [cited 2021 Apr 30];23:200120. Available from: https://www.sciencedirect.com/science/article/pii/S2666149721000025
Yisak H, Ewunetei A, Kefale B, Mamuye M, Teshome F, Ambaw B, et al. Effects of Vitamin D on COVID- 19 Infection and Prognosis: A Systematic Review. Risk Manag Healthc Policy. 2021;14:31-8.
Nogues X, Ovejero D, Pineda-Moncusí M, Bouillon R, Arenas D, Pascual J, et al. Calcifediol treatment and COVID-19-related outcomes. J Clin Endocrinol Metab [Internet]. [cited 2021 Jun 9]; Available from: https://academic.oup.com/jcem/advance-article/doi/10.1210/clinem/dgab405/6294179
July 2020 study by Linda Benskin* Massive Review of papers on Vitamin D and COVID-19 - July 3, 2020 *---
Vitamin D Life
A later COVID and Vitamin D book by Anderson and Grimes - Sept 2023
Previous book: Vitamin D Deficiency and Covid-19: Book by Drs Anderson and Grimes - July 2020
Mortality and Virus
{category}
Vitamin D meta-analyses for Virus
{category}
COVID-19 treated by Vitamin D - studies, reports, videos
- {include}
30 most recently changes Virus items
{LISTPAGES}
Vitamin D levels can be quickly restored by one or more loading doses* Loading Dose of Vitamin D category has the following *{include}
It appears that the body responds in a few hours to nanoemulsion Vitamin D under the tongue
Bioavailability of nanoemulsion formulations of Vitamin D3 – Nov 2019
COVID-19 defeated 3x faster by 420,000 IU Vitamin D nanoemulsion – RCT Nov 12, 2020
Vitamin D nanoemulsion etc. for fortification, pills, injections, topical and cancer – July 2019