Overview Liver and vitamin D
Summary
Fact: A properly functioning liver is needed for the efficient activation of vitamin D in the body
Fact: Liver diseases often result in lower levels of vitamin D
Fact: Various pain relievers damage the liver function
Fact: Lower levels of vitamin D result in osteoporosis and many other diseases
Options with a poorly functioning liver appear to be:
Increased vitamin D (example: 2X more vitamin D if Liver is 1/2 as efficient)
Consider supplementing with Iron - a patented Iron supplement appears to work very well
Get prescription for active form of vitamin D ( Calcitriol ) which does not need the liver or kidney to get the benefits of vitamin D in the body
Get Calcidiol which does not need the liver
Use Topical Vitamin D - activation by the skin etc does not require the liver
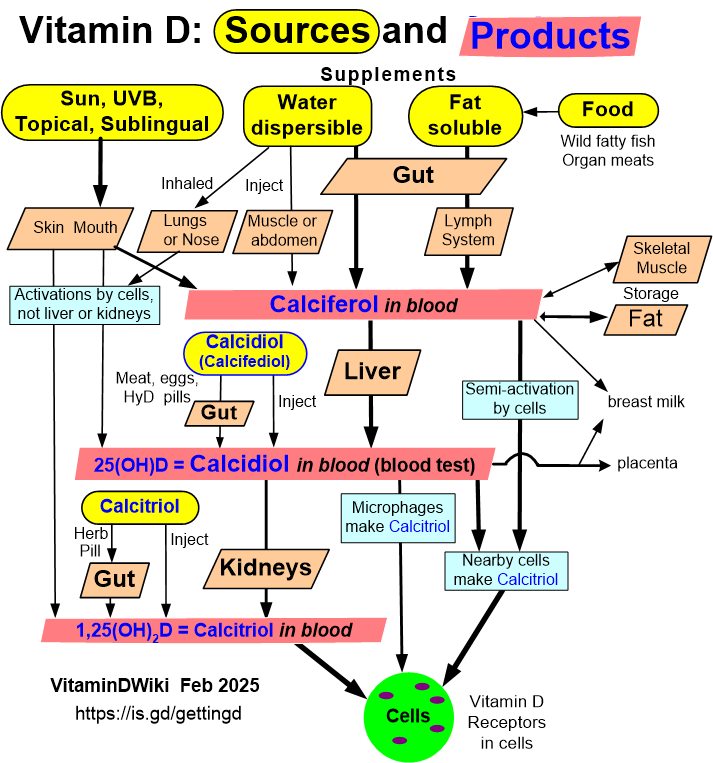
Click on image for ways of getting vitamin D even if Liver is not functioning well
How Acetaminophen causes liver failure
Acetaminophen is normally metabolized in the liver through two safe pathways (glucuronidation and sulfation). However, a small fraction is processed by the CYP2E1 enzyme into a toxic metabolite called NAPQI (N-acetyl-p-benzoquinone imine). Under normal doses, NAPQI is quickly neutralized by glutathione. When glutathione stores are depleted — through overdose or other risk factors — NAPQI accumulates and directly destroys liver cells (hepatocytes).
Key Numbers
- Acetaminophen overdose accounts for roughly ~50% of all acute liver failure cases in the U.S.
- It causes approximately ~500 deaths per year in the U.S. and tens of thousands of hospitalizations.
- The therapeutic dose is up to 4g/day for healthy adults; toxicity can occur at 7.5–10g+ in a single dose, and at much lower doses in high-risk individuals.
Risk Factors That Lower the Threshold for Toxicity
| Factor | Why It Matters |
|---|---|
| Chronic alcohol use | Induces CYP2E1 (more NAPQI) and depletes glutathione |
| Fasting / malnutrition | Depletes glutathione stores |
| Liver disease | Reduced metabolic capacity |
| Certain drugs (e.g., isoniazid, rifampin) | CYP2E1 inducers |
| CYP2E1 genetic variants | Faster NAPQI production |
Treatment
The antidote is N-acetylcysteine (NAC), which replenishes glutathione. It is highly effective if given early (within 8–10 hours of ingestion), but outcomes worsen significantly with delayed treatment.
Vitamin D and Liposomal Glutathione can both reduce Liver failure
Acetaminophen (APAP) overdose is the leading cause of acute liver failure in many countries, acting through oxidative stress and inflammation triggered by its toxic metabolite NAPQI and the resulting glutathione depletion.
Vitamin D Deficiency Makes It Worse (noticed first in mice)
Multiple studies have confirmed that vitamin D3 protects against APAP-induced acute liver injury (ALI). Research specifically examining vitamin D deficiency (VDD) found that a sublethal dose of APAP caused only slight liver enzyme elevations in normal mice — but those elevations were significantly aggravated in VDD-fed mice. Hepatic necrosis, hepatocyte death, glutathione depletion, and lipid peroxidation were all exacerbated in the vitamin D-deficient group.
Vitamin D3 Is Protective — Even Reduces Mortality
In a controlled mouse study, APAP administration caused significant liver enzyme elevation, inflammatory cytokines (TNF-α and IL-6), glutathione depletion, and oxidative stress — and 25% of the APAP-only mice died. In the calcitriol (VD3) treated group, there were zero deaths, along with significantly reduced liver enzymes, inflammation markers, and restored glutathione levels.
Protects in 3 ways
Vitamin D protects the liver from APAP toxicity through at least three pathways:
Antioxidant restoration — Vitamin D helps restore glutathione reserves, reduces lipid peroxidation, and supports antioxidant enzymes including glutathione peroxidase, catalase, and superoxide dismutase.
Anti-inflammatory action — Vitamin D modulates the NrF2/BACH1/HO-1 pathway, reducing NF-κB-driven inflammation, TNF-α, and oxidative stress mediators in both liver and kidney tissue.
VDR signaling disruption by APAP — APAP toxicity itself alters the hepatic expression of vitamin D-metabolizing enzymes (CYP2R1, CYP27B1, CYP24A1), its receptor (VDR), and binding protein (VDBP) — meaning overdose actively disrupts vitamin D signaling in the liver.
Vitamin D Is Safe for the Liver
Importantly, neither normal nor excessively high intakes of vitamin D are associated with liver injury or liver test abnormalities. Although hepatocytes, cholangiocytes, stellate cells and resident immune cells all have vitamin D receptors, there is no evidence that vitamin D itself causes liver injury.
Glutathione and NAC also help
Worth noting for the page: both vitamin D and NAC protect against APAP toxicity by preserving/restoring glutathione — vitamin D through VDR-mediated antioxidant gene expression, and NAC as a direct glutathione precursor. Your existing glutathione supplementation content on Vitamin D Life connects well here.
Renamed NAFLD => MASLD; NASH => MASH July 2023
NAFLD renamed July 2023 ==> metabolic dysfunction–associated steatotic liver disease = MASLD
Also renamed NASH ==> Metabolic dysfunction–associated steatohepatitis, or MASH
Both renamings the result of 3-year effort involving some 236 panelists from 56 countries
See Vitamin D Life
Liver Category
Vitamin D Life pages with NON-ALCOHOLIC or NAFLD in title (24 pages as of July 2023)
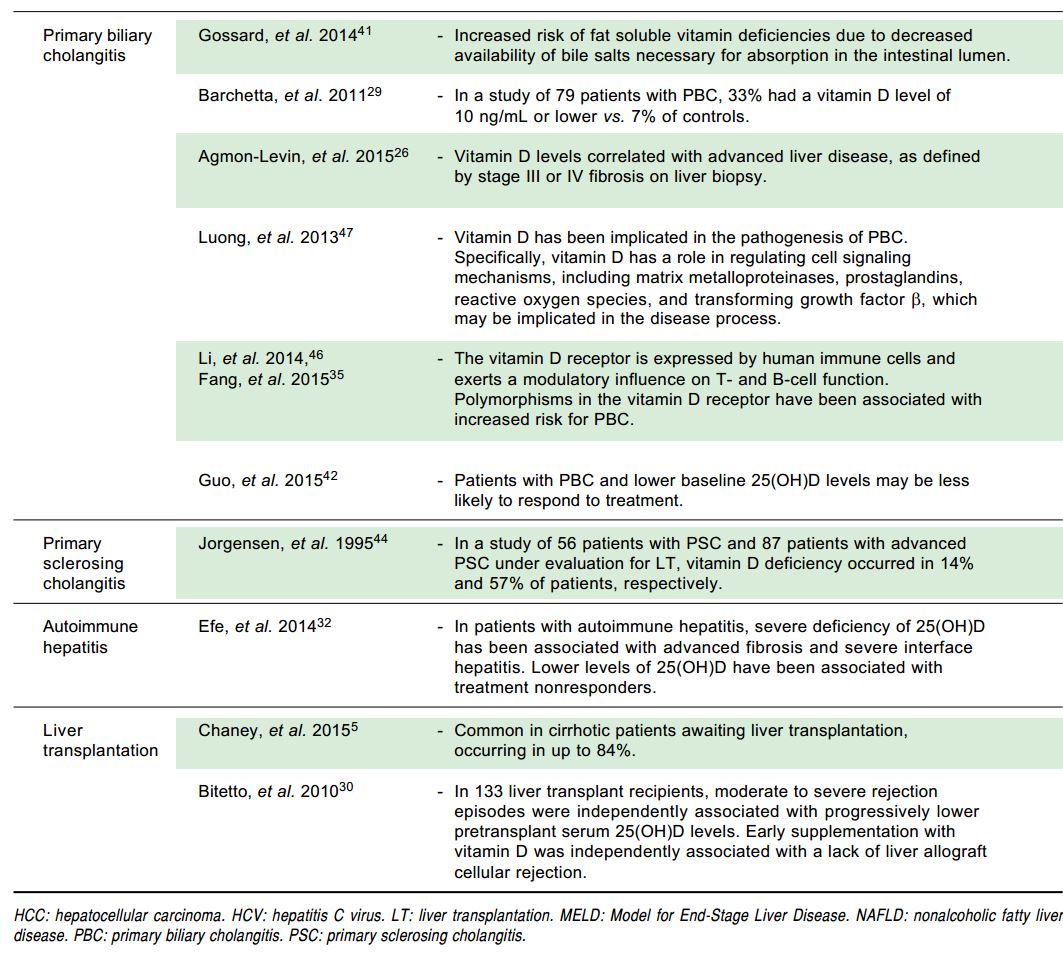
Hepatitis C, non-alcoholic fatty liver disease and vitamin D deficiency – Dec 2014 great summary tables
Important interactions between the liver and vitamin D – May 2013 excellent, with lots of graphs and tables
Advanced liver cirrhosis death 6.3X more likely if extremely low vitamin D – Jan 2013
Vitamin C reduces liver inflammation, which improves vitamin D production – Dec 2014
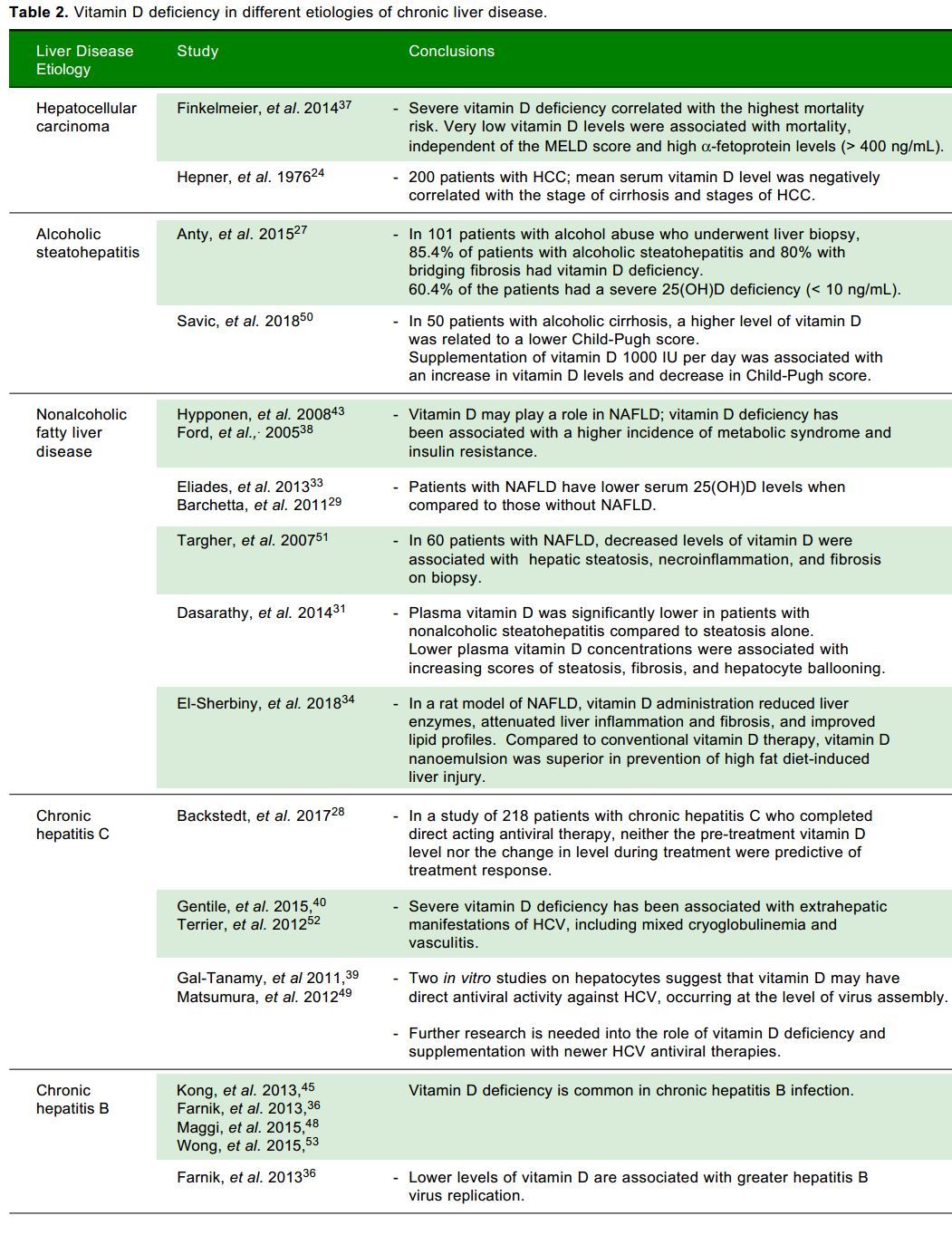
The worse the chronic liver disease, the lower the vitamin D level – Review Dec 2012
Death due to liver problems was 4X more probable with low levels of vitamin D – May 2012
Liver injury associated with low level of vitamin D – April 2011
Alcoholics with low vitamin D get more bone fractures – Jan 2011
Magnesium and vitamin D Alcohol uses up Magnesium, which is needed for bone strength
Vitamin D intervention stopped bone loss in mice getting too much alcohol – Aug 2012
Pharmacology of vitamin D - April 2011 many details on Calcidiol by Glossman
Vitamin D Deficiency and Liver Disease – Aug 2010 Question and Answer format
- Calcidiol , which does not require hydroxylation by the liver can be taken in place of vitamin D
Calcidiol may be 5X more effective than Vitamin D3 – June 2012
Calcidiol (produced by Liver, etc.) category listing has items along with related searches
Active form of vitamin D ( Calcitriol ) cut in half the fractures following organ transplant – meta-analysis Aug 2011
Calcitriol is available by prescription onlyOral vitamin D replacement is effective in chronic liver disease. – Aug 2010
Just give more vitamin D if the liver is still somewhat functioning
Overview Loading dose for vitamin D some people like to refill vitamin D levels quickly- Loading doses should be appropriate for those with liver problems
25-Hydroxyvitamin D3 suppresses hepatitis C virus production – Oct 2012
Hepatitis-C both treated and prevented by Vitamin D (many studies
Graphs of diseases vs vitamin D levels - April 2011 has the following

Inflammatory diseases: review of vitamin D, with many tables – May 2014 which has a summary table
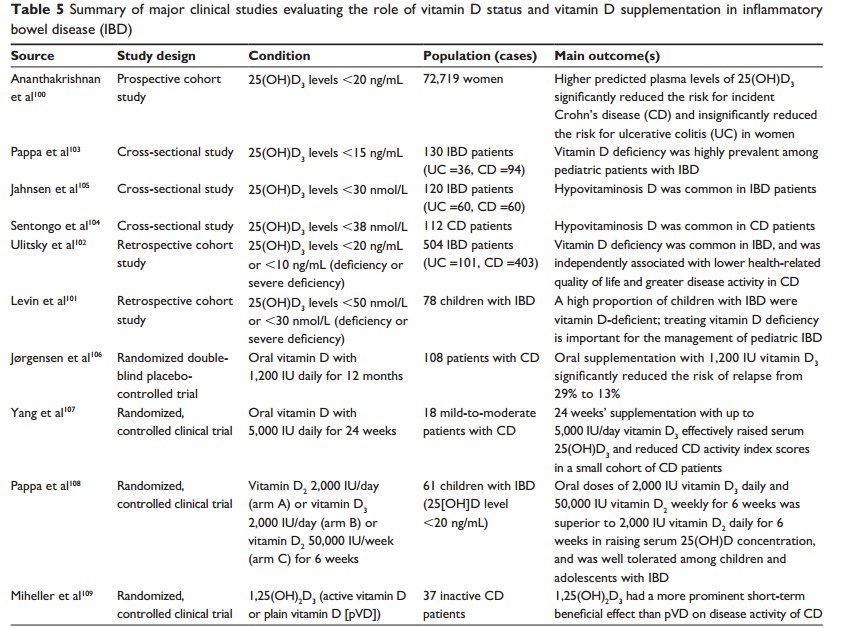
Most of the people with the diseases have less than 20 ng of vitamin D
See also Web
Wikipedia nonalcoholic fatty liver disease, April 2021
"Over 90% of obese, 60% of diabetic, and up to 20% normal-weight people develop it"
"NAFLD is the most common liver disorder worldwide and is present in approximately 25% of the world's population"
"In the United States, estimates suggest between 30 and 40% of adults have NAFLD,"
"The name "non-alcoholic steatohepatitis" (NASH) was later defined in 1980" at Mayo Clinic
"...NAFLD term started to be used around 2002"
More Than 90% of Patients of Cirrhosis Have Vitamin D Deficiency: A Cross-section Study June 2015
PubMed alcohol "vitamin d" Feb 2015 258 items – examples follow
- Role of obesity , alcohol and smoking on bone health 2012
- Association of 25-hydroxyvitamin D levels with liver dysfunction and mortality in chronic liver disease – 2012
- die more quickly if so much alcohol then liver dysfunction and low vitamin D
- Assessing bone status in patients awaiting liver transplantation – 2011 88% had low vitamin D levels
- What People Recovering from Alcoholism Need to Know About Osteoporosis NIH
Acetaminophen is involved in the most common cause of acute liver failure in adults Nov 2011 full text on-line
High Risk Groups for Poor Vitamin Status includes Alcohol
Alcohol and Other Factors Affecting Osteoporosis Risk in Women with bone photos - from 2003
EHow:Vitamin D & Liver Function
- Vitamin D is not considered an essential vitamin for liver function, but liver function is essential to providing vitamin D to the body.
Vitamin D deficiency in chronic liver disease Dec 2014
- "Published studies provide evidence for routine screening for hypovitaminosis D in patients with liver disease"
- Adverse Effects of Vitamin D Deficiency on Outcomes of Patients With Chronic Hepatitis B. Oct 2014
- 1.9X more chronic hepatitis B events if low Vitamin D (publisher wants $30 for the PDF)
- 2800 IU of vitamin D did not help Cirrhotic Patients - RCT 2016 Nutrients Journal
- No surprise, full text online
- Obese military conscripts were 2X as likely to have liver disease 30 years later NYT March 2017
- Vitamin D deficiency in patients with liver cirrhosis - 2016
- Liver Damage Is a Growing Epidemic Mercola Aug 2018
- "Between 2000 and 2016, the annual death toll from liver cancer in the U.S. rose by 43 % for men and 40 % for women"
- "Between 2001 and 2013, diagnosed cirrhosis cases nearly doubled; deaths from cirrhosis increased by 65 % between 1999 and 2016."
- Vitamin D NOT mentioned
- "This Workhorse of an Organ Can’t Signal for Help – Until It’s Often Too Late" Mercola March 2019
- "That is, until it falls to about 10 percent of its healthy working capacity."
- " Fructose , the most damaging type of sugar to your body, is particularly hard on your liver, much like alcohol"
Should monitor Liver Cirrhosis for Vitamin D, A and Zinc - 2018
An Argument for Vitamin D, A, and Zinc Monitoring in Cirrhosis.
Ann Hepatol. 2018 Oct 16;17(6):920-932. doi: 10.5604/01.3001.0012.7192.
📄 Download the PDF from Vitamin D Life

Malnutrition is prevalent in cirrhosis. Vitamin and mineral deficiencies, including vitamin D, vitamin A, and zinc, are common and have been shown to correlate with survival. Our aim was to review the mechanisms of vitamin D, vitamin A, and zinc deficiencies in cirrhosis and the clinical assessment of affected patients, their outcomes based on the current literature, and management. This is a narrative review including the relevant literature for cirrhosis and vitamin D, vitamin A, and zinc deficiencies. Vitamin D deficiency has important effects in cirrhosis, regardless of the cause of chronic liver disease.These effects include associations with fibrosis and outcomes such as infections, hepatocellular carcinoma, and mortality. Vitamin A deficiency is associated with liver disease progression to cirrhosis and clinical decompensation, including occurrence of ascites or hepatic encephalopathy. Zinc deficiency can lead to hepatic encephalopathy and impaired immune function. Such deficiencies correlate with patient survival and disease severity. Caution should be applied when replacing vitamin D, vitamin A, and zinc to avoid toxicity. Identification and appropriate treatment of vitamin and mineral deficiencies in cirrhosis may reduce specific nutritional and cirrhosis-related adverse events. Routine monitoring of vitamin A, vitamin D and zinc levels in cirrhosis should be considered.
Chronic Liver Diseases might be treated by Vitamin D - Dec 2014
New insight of vitamin D in chronic liver diseases
Hepatobiliary Pancreat Dis Int. 2014 Dec;13(6):580-5. PMID: 25475859
Chen EQ1, Shi Y, Tang H.
CONCLUSIONS:
Although the exact role and mechanisms of vitamin D have not been fully elucidated in chronic liver diseases,
it is potentially beneficial in the treatment of chronic liver diseases.
Further mechanistic studies are needed to validate its clinical application.
📄 Download the PDF from Vitamin D Life.
Low vitamin D = 2X worse liver cancer prognosis
Severe 25-hydroxyvitamin D deficiency identifies a poor prognosis in patients with hepatocellular carcinoma - a prospective cohort study.
Aliment Pharmacol Ther. 2014 May;39(10):1204-12. doi: 10.1111/apt.12731. Epub 2014 Mar 29.
Finkelmeier F1, Kronenberger B, Köberle V, Bojunga J, Zeuzem S, Trojan J, Piiper A, Waidmann O.
BACKGROUND: Vitamin D is involved in many biological processes. The role of vitamin D in patients with hepatocellular carcinoma (HCC) remains inconclusive, although there is evolving evidence that vitamin D may modulate cancer development and progression.
AIM: To evaluate serum vitamin D as prognostic parameter in HCC, we performed a prospective cohort study.
METHODS: HCC patients were prospectively recruited and 25-hydroxyvitamin D3 (25(OH)D3 ) levels were determined. 25(OH)D3 levels were compared to stages of cirrhosis and HCC stages with nonparametric Kruskal-Wallis tests and Spearman correlations in 200 HCC patients. The association of the 25(OH)D3 levels and overall survival (OS) was assessed in uni- and multivariate Cox regression models.
RESULTS: Two-hundred patients with HCC were included. The mean follow-up time was 322 ± 342 days with a range of 1-1508 days. Nineteen patients underwent liver transplantation and 60 patients died within the observation time. The mean serum 25(OH)D3 concentration was 17 ± 13 ng/mL with a range of 1-72 ng/mL. 25(OH)D3 serum levels negatively correlated with the stage of cirrhosis as well as with stages of HCC. Patients with severe 25(OH)D3 deficiency had the highest mortality risk ( hazard ratio 2.225 , 95% confidence interval 1.331-3.719, P = 0.002). Furthermore, very low 25(OH)D3 levels were associated with mortality independently from the MELD score and high alpha-Fetoprotein levels (>400 ng/mL) in a multivariate Cox regression model.
CONCLUSIONS: We conclude that 25(OH)D3 deficiency is associated with advanced stages of hepatocellular carcinoma and it is a prognostic indicator for a poor outcome.
Progression of Liver damage
NAFLD inversely related to Vitamin D only in whites - Sept 2019
Serum 25-hydroxyvitamin-D and nonalcoholic fatty liver disease: Does race/ethnicity matter? Findings from the MESA cohort
Nutr Metab Cardiovasc Dis. 2019 Sep 10. pii: S0939-4753(19)30342-4. doi: 10.1016/j.numecd.2019.09.004
El Khoudary SR1, Samargandy S2, Zeb I3, Foster T4, de Boer IH5, Li D6, Budoff MJ7.
BACKGROUND AND AIMS:
Low serum 25-hydroxyvitamin D (25(OH)D) is associated with higher nonalcoholic fatty liver disease (NAFLD) risk in studies of mainly white participants. Significant racial/ethnic differences exist in serum 25(OH)D and NAFLD prevalence questioning extending this association to other racial/ethnic groups. We tested whether the association between serum 25(OH)D and NAFLD vary by race/ethnicity.
METHODS AND RESULTS:
This was a cross-sectional analysis from the Multi-Ethnic Study of Atherosclerosis (MESA) that included 3484 participants (44% male; 38.4% Whites, 27.8% African-Americans, 23.5% Hispanics, and 10.3% Chinese-Americans) who had serum 25(OH)D and upper abdominal CT images available at baseline. Serum 25(OH)D was measured by high-performance liquid chromatography-tandem mass spectrometry. NAFLD was identified if liver-to-spleen Hounsfield-Unit ratio was <1. Whites had the highest 25(OH)D level and African-Americans had the lowest level (mean ± SD: 29.5 ± 10.4 vs.19.9 ± 9.1, respectively). Six hundred and eleven (17.5%) participants had NAFLD;
Hispanics had the highest prevalence (26.2%) followed by
Chinese-Americans (19.8%),
Whites (15.8%) and
African-Americans (11.7%), P < 0.0001.
In adjusted model, the association of 25(OH)D with NAFLD differed by race/ethnicity (P < 0.0001). Negative association was only evident in Causations (OR (95% CI):1.23 (1.03, 1.47) per 1 SD lower serum 25(OH)D). For other racial/ethnic groups, BMI, triglycerides, diabetic status and/or smoking, but not serum 25(OH)D, were common independent risk factors for NAFLD.
CONCLUSIONS:
The negative association between serum 25(OH)D and NAFLD in Whites may not be broadly generalizable to other racial/ethnic groups. Modifiable risk factors including BMI, triglycerides, diabetic status and/or smoking associated with NAFLD risk in non-white racial/ethnic groups beyond 25(OH)D.
Liver factoids from The Body, by Bill Bryson, 2019
The liver takes part in some five hundred metabolic processes.
2/3 of the liver can be removed and it regenerates
third of us are thought to have early stages of NAFLD, but luckily for most of us it never progresses beyond that.
* NAFLD is starting to be found in young children—somewhere it had never been seen before until recently. An estimated 10.7 percent of US children
Hepatitis C can live within victims for forty years or more, stealthily demolishing their livers, without their being aware of it. The CDC estimates that if all those people could be identified and treated, 120,000 lives would be saved in America alone.
Alcohol-Related Liver Disease might be associated with Low Mg, Vitamin D, Zinc, Selenium - Sept 2021
The Role of Micronutrients in the Pathogenesis of Alcohol-Related Liver Disease
Alcohol Alcohol. 2021 Sep 7;agab060. doi: 10.1093/alcalc/agab060
Ruairidh Nicoll 1, Konstantinos Gerasimidis 2, Ewan Forrest 1
Aims: Chronic alcohol consumption may result in liver injury and chronic liver disease, but other factors are likely to influence disease progression. Malnutrition, specifically micronutrient deficiency, is frequently associated with both alcohol use disorder and chronic liver disease. We hypothesize that micronutrient deficiencies may affect the progression of liver disease in this population.
Methods: Systematic integrative review of the medical literature; electronic search of MEDLINE 1950-2021; studies investigating role of any micronutrient in the acceleration of alcohol-related liver injury in humans or animals. Studies which specifically related to alcoholic hepatitis were excluded. Outcomes were extracted and recorded in tabulated form and discussed narratively.
Results: We identified 46 studies investigating the role of micronutrient deficiencies in the pathogenesis of alcohol-related liver disease. Specific micronutrients which were identified included folic acid or related B vitamins (n = 9 studies), Vitamin D (n = 9 studies), magnesium (n = 8 studies), zinc (n = 8 studies) and selenium (n = 12 including one systematic review). Observational evidence suggests a potential role of magnesium deficiency in accelerating alcohol-related liver injury with weak or negative evidence for other micronutrients.
Conclusions: Magnesium deficiency may increase the risk of alcohol-related liver injury and adverse liver outcomes. However, currently, there is insufficient evidence to support magnesium supplementation except for clinically relevant magnesium deficiency. Long-term prospective cohort studies assessing the impact of micronutrients on liver disease progression in patients with alcohol use disorder are lacking and may help determine whether there is a causal role for micronutrient deficiencies in alcohol-related liver injury.