Vitamin D Intake May Reduce SARS-CoV-2 Infection Morbidity in Health Care Workers
Tatiana L. Karonova *'[email protected], Alena T. Chernikova , Ksenia A. Golovatyuk 1, Ekaterina S. Bykova 1, William B. Grant , Olga V. Kalinina 1, Elena N. Grineva 1 and Evgeny V. Shlyakhto 1
Clinical Endocrinology Laboratory, Department of Endocrinology, Almazov National Medical Research Centre, 194021 Saint Petersburg, Russia; arabicaa at gmail.com (A.T.C.); ksgolovatiuk at gmail.com (K.A.G.); bykova160718 at gmail.com (E.S.B.); olgakalinina at mail.ru (O.V.K.); grineva_e at mail.ru (E.N.G.); shlyakhto_ev at almazovcentre.ru (E.V.S.)
Sunlight, Nutrition, and Health Research Center, P.O. Box 641603, San Francisco, CA 94164-1603, USA; williamgrant08 at comcast.net
Abstract
In the last 2 years, observational studies have shown that a low 25-hydroxyvitamin D (25 ( OH )D) level affected the severity of infection with the novel coronavirus (COVID-19). This study aimed to analyze the potential effect of vitamin D supplementation in reducing SARS-CoV-2 infection morbidity and severity in health care workers. Of 128 health care workers, 91 (consisting of 38 medical doctors (42%), 38 nurses (42%), and 15 medical attendants (16%)) were randomized into two groups receiving vitamin D supplementation.
- Participants of group I (n = 45) received water- soluble cholecalciferol at a dose of 50,000 IU/week for 2 consecutive weeks, followed by 5000 IU/day for the rest of the study.
- Participants of group II (n = 46) received water-soluble cholecalciferol at a dose of 2000 IU/day.
For both groups, treatment lasted 3 months. Baseline serum 25(OH)D level in health care workers varied from 3.0 to 65.1 ng/mL (median, 17.7 (interquartile range, 12.2; 24.7) ng/mL). Vitamin D deficiency, insufficiency, and normal vitamin D status were diagnosed in 60%, 30%, and 10%, respectively. Only 78 subjects completed the study. Vitamin D supplementation was associated with an increase in serum 25(OH)D level, but only intake of 5000 IU/day was accompanied by normalization of serum 25(OH)D level, which occurred in 53% of cases. Neither vitamin D intake nor vitamin D deficiency/insufficiency were associated with a decrease in SARS-CoV-2 morbidity (odds ratio = 2.27; 95% confidence interval, 0.72 to 7.12).
However, subjects receiving highdose vitamin D had only asymptomatic SARS-CoV-2 in 10 (26%) cases; at the same time, participants who received 2000 IU/day showed twice as many SARS-CoV-2 cases, with mild clinical features in half of them.
Download the PDF from Vitamin D Life
Note: Medical Attendants had very low initial levels. Wonder why
Discussion
To our knowledge, this is the first randomized interventional trial among health care workers to show that high-dose vitamin D supplementation is safe and effective in achieving normal vitamin D levels, but was not connected to reduced SARS-CoV-2 morbidity. However, intake of 50,000 IU/week twice, followed by 5000 IU/day, seemed to be associated with asymptomatic COVID-19 cases, whereas health care workers receiving 2000 IU/day had a two-fold higher infection that was symptomatic with mild clinical features in half of cases.
Vitamin D is postulated to play an important immunomodulatory role, and deficiency is associated with increased incidence of ARVI, including COVID-19 [26-28]. Our previous results also showed that severe vitamin D deficiency is associated with severity and death in COVID-19 patients [29], and were comparable to recent findings [4,30]. Dis- sanayake and colleagues, whose meta-analysis included 72 COVID-19 observational and 4 interventional randomized studies, have shown not only correlations between 25(OH)D level and severity or mortality, but also some clinical benefits and improvement in inflammatory markers of vitamin D supplementation in treating COVID-19 [22].
Recent observational studies showed a more frequent vitamin D deficiency among shift workers and newcomers, including health care workers, than day workers [17,31,32], whereas data regarding mortality rate showed a high COVID-19-related mortality among health care workers, as published by the World Health Organization [33]. Thus, a great necessity exists to find new effective measures to prevent SARS-CoV-2 and/or decrease COVID-19 morbidity and severity in medical workers. Taking into account the need to improve preventive actions for medical staff in daily contact with SARS-CoV-2 patients, we developed a hypothesis for this research to assess vitamin D supplementation's effectiveness in preventing COVID-19 among this population.
To reduce the risk of infection, it is recommended that people at risk should rapidly increase 25(OH)D concentrations above 40-60 ng/mL [27,34]. In order to achieve this, patients need to take higher loading vitamin D doses: 100,000-200,000 IU over 8 weeks [34,35]. To maintain that level after the first month, the dose can be decreased to 5000 IU/day [36]. Considering published recommendations for decreasing the morbidity of COVID-19 [27,34,35], we have chosen a high vitamin D supplementation dose of 50,000 IU/week twice for a rapid increase of 25(OH)D level, followed by 5000 IU/day, and compared with the common daily dose used in clinical practice. We showed a good tolerability of the saturating dose of water-soluble cholecalciferol, and a rapid increase in the serum 25(OH)D level to normal values without an increase in total calcium levels in the blood. Those results are comparable to those of previous works [36,37].
Inspection of the population-based study results shows that subjects with cholecalciferol supplementation had a lower risk of SARS-CoV-2 infection (hazard ratio (HR) = 0.95 (95% CI, 0.91 to 0.98); p = 0.004) than deficient unsupplemented subjects. The protective effect was more significant between treated subjects with 25(OH)D > 30 ng/mL and untreated deficient subjects (HR = 0.57 (95% CI, 0.50 to 0.66); p < 0.001) [38]. In our study, no significant differences were evident in morbidity between the comparable groups, and no difference in serum 25(OH)D level emerged between subjects with positive or negative IgG titers despite vitamin D supplementation. That result might be related to our inability to achieve the recommended 25(OH)D level of 40-60 ng/mL. However, subjects receiving a higher dose of cholecalciferol had an asymptomatic course of viral infection. Those differences can be explained by engagement mechanisms as in the cell-bound and adaptive immunity, as well as a protective function on the level of upper-airway mucosa [39].
Possible study limitations include the small sample, absence of lab baseline data of serum 25(OH)D level and IgG before randomization, and short study duration of 3 months. In addition, the study was carried out in a comparative rather than placebo-controlled design. Therefore, conducting more detailed research is necessary to better understand vitamin D's role in preventing SARS-CoV-2 infection.
Vitamin D Life – COVID-19 treated by Vitamin D - studies, reports, videos
As of May 7, 2022, the Vitamin D Life page had: 34 trials, 10 trial results, 36 meta-analyses and reviews, 69 observations, 38 recommendations, 55 associations, 89 speculations, 58 videos, 45 Mortality studies see related: Governments, HealthProblems, Hospitals, Dark Skins, 26 risk factors are ALL associated with low Vit D, Recent Virus pages Fight COVID-19 with 50K Vit D weekly Vaccines Take lots of Vitamin D at first signs of COVID
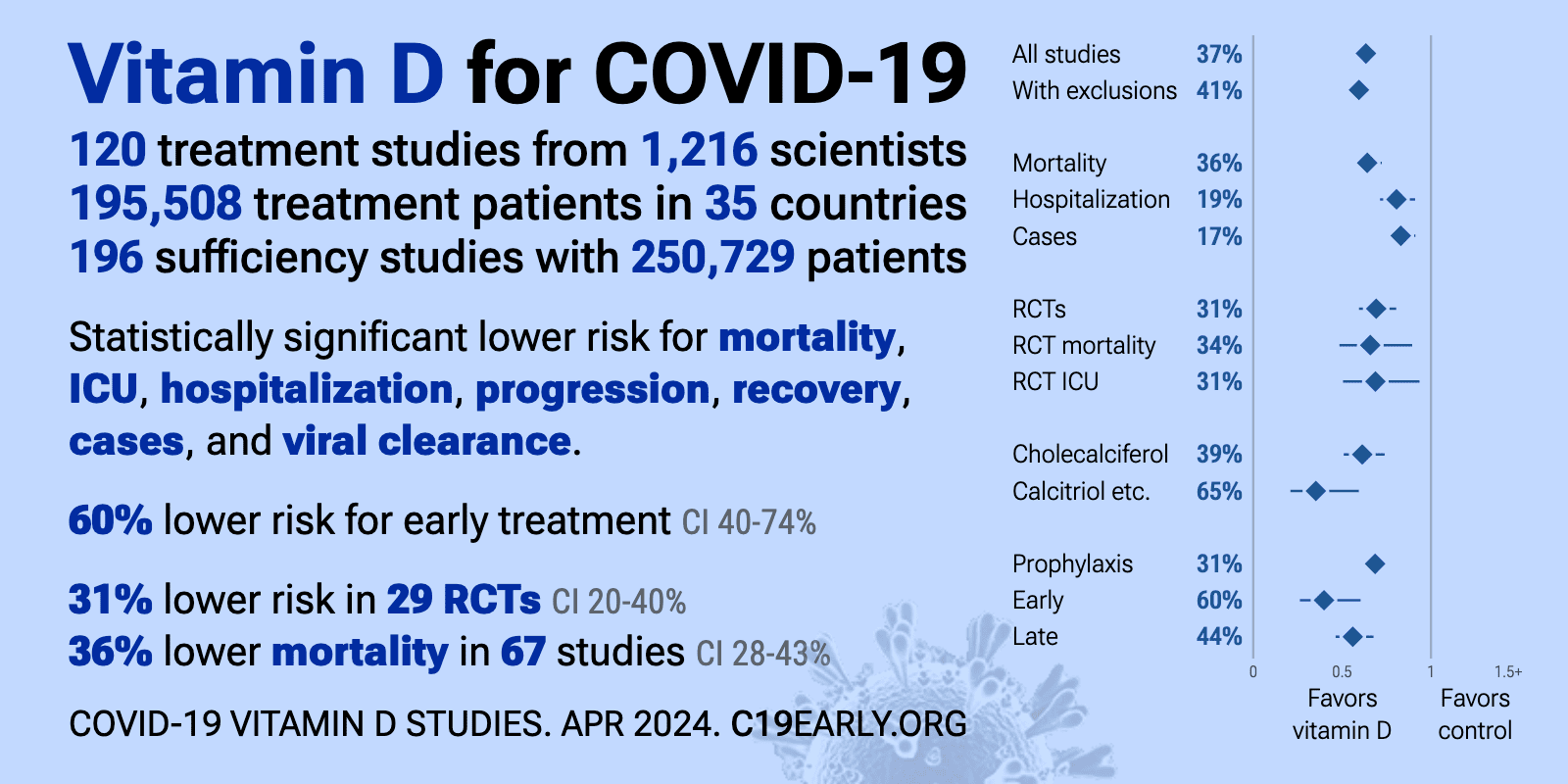
- The above image is automatically updated