Knee osteoarthritis helped by Low Level Laser Therapy
Judy, the wife of the founder of Vitamin D Life, is getting osteoarthritis pain in both of her knees
Founder had made LLLT device for her post-breast cancer lymphoedema
That LLLT worked extremely well for 10 years
It used pulsed rather than continuous light (as analyzed by meta-analysis on this page)
We are trying to use that LLLT for her knee Osteoarthritis as of Nov 2019
We know that LLLT works, but do not know why
Possible reasons include:
Provides energy to the cells
Creaates NO2 or Vitamin D in the cells
Increases circulation
See LLLT in Vitamin D Life
LLLT reverses Age-related Macular Degeneration for a while - multiple studies
Off topic: Low Level Laser Therapy works - makes Nitric Oxide and ATP
- Which includes: 45 LLLT benefits March 2019
LLLT treated founder's knee osteoarthritis flareup in just 2 days
Low Level Laser therapy and photobiomodulation proven to help health for many years – May 2020
Osteoarthritis category includes the following
{include}
RCT 2012 - lots of benefit, also observed 1/2 degree temperature rise
Efficacy of low-level laser therapy associated with exercises in knee osteoarthritis: a randomized double-blind study
Clinical Rehabilitation, https://doi.org/10.1177/0269215511425962
Patrícia Pereira Alfredo, Jan Magnus Bjordal, Sílvia Helena Dreyer, ...
Objectives: To estimate the effects of low level laser therapy in combination with a programme of exercises on pain, functionality, range of motion, muscular strength and quality of life in patients with osteoarthritis of the knee.
Design: A randomized double-blind placebo-controlled trial with sequential allocation of patients to different treatment groups.
Setting: Special Rehabilitation Services.
Subjects: Forty participants with knee osteoarthritis, 2–4 osteoarthritis degree, aged between 50 and 75 years and both genders.
Intervention: Participants were randomized into one of two groups: the laser group (low level laser therapy dose of 3 J and exercises) or placebo group (placebo laser and exercises).
Main measures: Pain was assessed using a visual analogue scale (VAS), functionality using the Lequesne questionnaire, range of motion with a universal goniometer, muscular strength using a dynamometer, and activity using the Western Ontario and McMaster Universities Osteoarthritis (WOMAC) questionnaire at three time points: (T1) baseline, (T2) after the end of laser therapy (three weeks) and (T3) the end of the exercises (11 weeks).
Results: When comparing groups, significant differences in the activity were also found (P = 0.03). No other significant differences (P > 0.05) were observed in other variables. In intragroup analysis, participants in the laser group had significant improvement, relative to baseline, on
pain (P = 0.001),
range of motion (P = 0.01),
functionality (P = 0.001) and
activity (P < 0.001).
No significant improvement was seen in the placebo group.
Conclusion: Our findings suggest that low level laser therapy when associated with exercises is effective in yielding pain relief, function and activity on patients with osteoarthritis of the knees.
📄 Download the PDF from Vitamin D Life
RCT March 2014 high intensity and exercise
High-intensity versus low-level laser therapy in the treatment of patients with knee osteoarthritis: a randomized controlled trial
Lasers in Medical Science, July 2014, V 29, # 4, pp 1371–1376, https://doi.org/10.1007/s10103-014-1529-0
Abdullah Raddah Kheshie Mohamed Salaheldien Mohamed Alayat Mohamed Mohamed Ebrahim Ali
The aim of this randomized controlled study was to compare the effects of low-level laser therapy (LLLT) and high-intensity laser therapy (HILT) on pain relief and functional improvement in patients with knee osteoarthritis (KOA). A total of 53 male patients participated in this study, with a mean (SD) age of 54.6 (8.49) years. Patients were randomly assigned into three groups and treated with HILT and exercise (HILT + EX), LLLT and exercise (LLLT + EX), and placebo laser plus exercise (PL + EX) in groups 1, 2, and 3, respectively. The outcomes measured were pain level measured by visual analog scale (VAS) and knee function measured by Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC). Statistical analyses were performed to compare the differences between baseline and posttreatment measurements. The level of statistical significance was set as P < 0.05. The result showed that HILT and LLLT combined with exercise were effective treatment modalities in decreasing the VAS and WOMAC scores after 6 weeks of treatment. HILT combined with exercises was more effective than LLLT combined with exercises, and both treatment modalities were better than exercises alone in the treatment of patients with KOA.
📄 Download the PDF from Sci-Hub via Vitamin D Life
LLLT + Exercise RCT 2019 - benefits continue and increase months after treatment
Exploring the efficacy of low-level laser therapy and exercise for knee osteoarthritis
South African Journal of Sports Medicine http://dx.doi.org/10.17159/2078-516x/2019/v31i1a6058
A KholvadiaI; D ConstantinouII; P J-L Gradidge
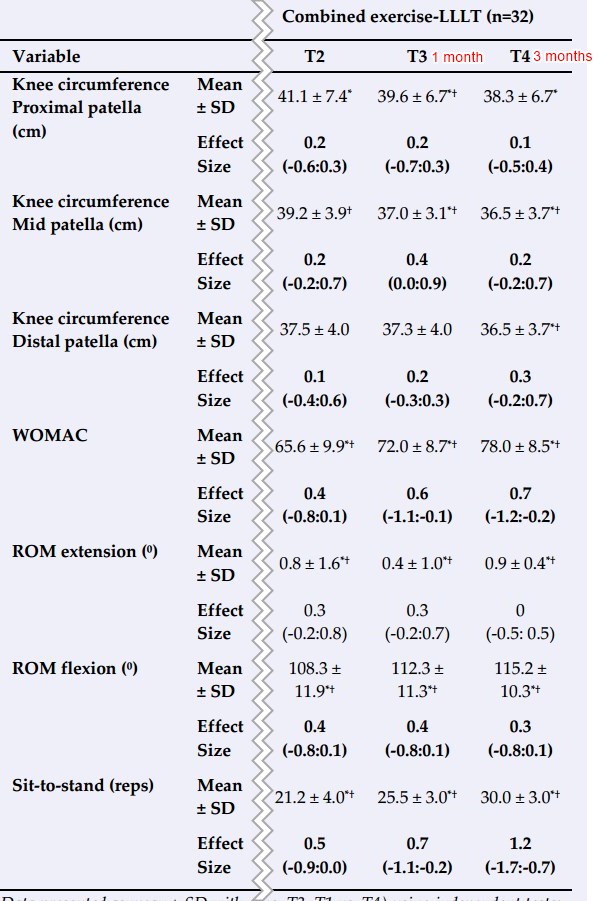
Some Treatment benefits were still increasing 3 months later
BACKGROUND: Knee Osteoarthritis (KOA) is a prevalent, chronic disorder with excessive functional, social and economic burdens. The goal of treatment is to alleviate the symptoms and slow the progression. Documenting the effects of exercise and LLLT as co-modalities in the management of KOA allows practitioners to implement this management tool as part of KOA rehabilitation, resulting in the earlier discharge from a supervised rehabilitation setting
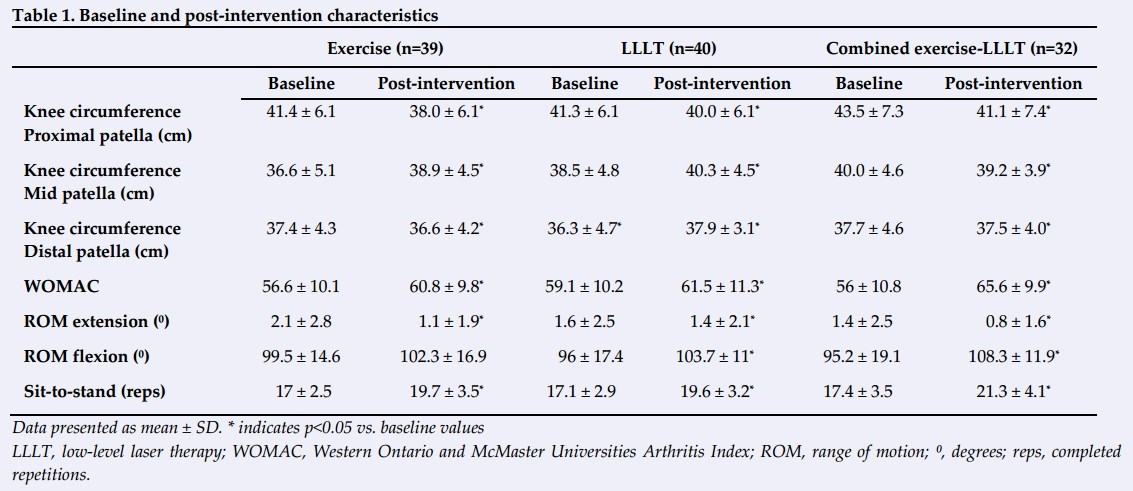
OBJECTIVE: The purpose of this study was to determine the effect of low-level laser therapy (LLLT) in the treatment of knee osteoarthritis (KOA). A randomised controlled trial (RCT) was conducted on 111 participants (aged between 40-75 years) diagnosed with KOA. Participants were randomised into an exercise (n=39), LLLT (n=40), or a combined exercise-LLLT (n=32) group
METHODS: The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scale was used to assess pain and functionality. Knee range of motion was assessed using a goniometer, and the one-minute timed sit-to-stand test measured physical functionality at four time points: (T1) baseline, (T2) post 12-session intervention, (T3) one-month post intervention and (T4) three-month's post intervention. Knee circumference was measured using a measuring tape
RESULTS: WOMAC pain and functionality scale and knee circumference scores decreased in all three groups (P<0.05), but the combined exercise-LLLT group demonstrated better outcomes than the LLLT or exercise alone groups respectively. The combined exercise-LLLT group showed better acute and long-term benefits with participants experiencing a 3.5 centimetre decrease in knee circumference, 24 point improvement in the WOMAC pain and functionality scale, and a four repetition increase in physical functionality
CONCLUSION: The findings suggest that LLLT is a viable tool for managing KOA when used in conjunction with physical exercise
📄 Download the PDF from Vitamin D Life
References
Felson DT, Lawrence RC, Dieppe RA, et al. Osteoarthritis: new insights. Part 1: the disease and its risk factors. Ann Intern Med 2000; 133(8):635-646 [doi: 10.7326/0003-4819-1339-200011070-00015]
Woolf AD. Global burden of osteoarthritis and musculoskeletal diseases. BMC Musculoskelet Disord 2015; 16(Suppl 1): S3. [doi: /10.1186/1471-2474-16-S1-S3]
Usenbo A, Kramer V, Young T, Musekiwa A. Prevalence of arthritis in Africa: A systematic review and meta-analysis. PLoS One 2015; 10(8): e0133858. doi:org/10.1371/journal.pone.0133858
Michael JW, Schlüter-Brust KU, Eysel P. The Epidemiology, Etiology, Diagnosis, and Treatment of Osteoarthritis of the Knee. Dtsch Arztebl Int 2010; 107(9): 152-162. [doi: 10.3238/arztebl.2010.0152]
Fransen M, McConnell S, Harmer AR, et al. Exercise for osteoarthritis of the knee: aCochrane systematic review. Br J Sports Med 2015; 49(24):1554-1557. [doi: 10.1136/bjsports-2015- 095424]
Alfredo PP, Bjordal JM, Junior WS, et al. Long-term results of a randomized, controlled, double-blind study of low-level laser therapy before exercises in knee osteoarthritis: laser and exercises in knee osteoarthritis. Clin Rehabil 2018; 32(2): 173178. [doi: 10.1177/0269215517723162]
Fukuda VO, Fukuda TY, Guimarâes M, et al. Short-term efficacy of low-level laser therapy in patients with knee osteoarthritis: a randomized placebo-controlled, double-blind clinical trial. Rev Bras Ortop 2015; 46(5): 526-533. [doi: 10.1016/S2255-4971(15)30407-9]
Alfredo PP, Bjordal JM, Dreyer SH, Meneses SRF, Zaguetti G, Ovanessian V, et al. Efficacy of low level laser therapy associated with exercises in knee osteoarthritis: a randomized double-blind study. Clin Rehabil. 2012; 26(6); 523-533. [doi: 10.1177/0269215511425962]
Bjordal, JM, Johnson, MI, Lopes-Martins RA, et al. Short-term efficacy of physical interventions in osteoarthritic knee pain: A systematic review and meta-analysis of randomized placebocontrolled trials. BMC Musculoskelet Disord 2007; 8:51. [doi: 10.1186/1471-2474-8-51]
Bülow, PM, Jensen, H, Danneskiold-Samsoe B. Low power GaAl-As laser treatment of painful osteoarthritis of the knee. A double-blind placebo controlled study. Scand J Rehabil Med 1994; 26(3): 155-159. [PMID: 7801065]
Jakobsen TL, Christensen M, Christensen SS, et al. Reliability of knee joint range of motion and circumference measurements after total knee arthroplasty: Does tester experience matter? Physiother Res Int 2010; 15(3): 126-134. [doi: 10.1002/pri.450]
Salaffi F, Leardini G, Canesi B, et al. Reliability and validity of the Western Ontario and McMaster Universities (WOMAC) Osteoarthritis Index in Italian patients with osteoarthritis of the knee. Osteoarthr Cartilage 2003; 11(8): 551-560. [doi: 10.1016/S1063-4584 (03)00089-X]
Huber EO, Meichtry A, de Bie RA, et al.. Construct validity of change scores of the Chair Stand Test versus Timed Up and Go Test, KOOS questionnaire and the isometric muscle strength test in patients with severe knee osteoarthritis undergoing total knee replacement. Man Ther 2016; 21: 262-267. [doi: 10.1016/j.math.2015.09.012]
Kahn F. Low Intensity Laser Therapy - in Clinical Practice. Meditech International , 2006: 44-45.
Williams VJ, Piva SR, Irrgang JJ, et al. Comparison of reliability and responsiveness of patient-reported clinical outcome measures in knee osteoarthritis rehabilitation. J Orthop Sports Phys Ther 2012; 42(8): 716-723. [doi: 10.2519/jospt.2012.4038].
Meta-analysis Sept 2015: 9 studies with continuous illumination found no benefit
- - they chose to not analyze the hundreds of studies which used modulated light
Effectiveness of low-level laser therapy in patients with knee osteoarthritis: a systematic review and meta-analysis
Osteoarthritis and Cartilage, Vol 23, Issue 9, Sept 2015, https://doi.org/10.1016/j.joca.2015.04.005
Huang J.Chen§aJ.Ma .Shen.Pei†V.B.Kraus
Note: There are a huge number of ways of modulating an LLLT
It appears that the benefit is proportional to the number of times the LLLT is turned on and off
It is virtually impossible to compare benefit of different modulations, so the meta-analysis ignored them
Also: Using very short pulses allows 100X stronger light intensity, which results in greater penetration depth
Objective
To investigate the efficacy of low-level laser therapy (LLLT) treatment of knee osteoarthritis (KOA) by a systematic literature search with meta-analyses on selected studies.
Design
MEDLINE, EMBASE, ISI Web of Science and Cochrane Library were systematically searched from January 2000 to November 2014. Included studies were randomized controlled trials (RCTs) written in English that compared LLLT (at least eight treatment sessions) with sham laser in KOA patients. The efficacy effective size was estimated by the standardized mean difference (SMD). Standard fixed or random-effects meta-analysis was used, and inconsistency was evaluated by the I-squared index (I2).
Results
Of 612 studies, nine RCTs (seven double-blind, two single-blind, totaling 518 patients) met the criteria for inclusion. Based on seven studies, the SMD in visual analog scale (VAS) pain score right after therapy (RAT) (within 2 weeks after the therapy) was not significantly different between LLLT and control (SMD = −0.28 [95% CI = −0.66, 0.10], I2 = 66%). No significant difference was identified in studies conforming to the World Association of Laser Therapy (WALT) recommendations (four studies) or on the basis of OA severity. There was no significant difference in the delayed response (12 weeks after end of therapy) between LLLT and control in VAS pain (five studies). Similarly, there was no evidence of LLLT effectiveness based on Western Ontario and McMaster Universities Arthritis Index (WOMAC) pain, stiffness or function outcomes (five and three studies had outcome data right after and 12 weeks after therapy respectively).
Conclusion
Our findings indicate that the best available current evidence does not support the effectiveness of LLLT as a therapy for patients with KOA.
📄 Download the PDF from Vitamin D Life
Vitamin D Life pages with LOW LEVEL LASER in title
This list is automatcially updated
{LIST()}
Title change made Nov 2020 caused the visitor count to reset.
There have actually been visitors to this page since it was originally made