High dose vitamin reduced pain of fibromyalgia, osteoarthritis, and rheumatoid arthritis
VITAMIN D STATUS AND THE EFFICACY OF HIGH-DOSE INTRAMUSCULAR CHOLECALCIFEROL ON MUSCULOSKELETAL PAIN AND MORNING FATIGUE IN PATIENTS WITH CHRONIC RHEUMATIC DISEASES
Ann Rheum Dis 2015;74(Suppl2): 307; DOI: 10.1136/annrheumdis-2015-eular.3877
B.Y. Choi1, S.H. Chang2, Y.W. Song3.
1Division of Rheumatology, Department of Internal Medicine, Seoul Medical Center, Seoul;
2Division of Rheumatology, Department of Internal Medicine, Soonchunhyang University Cheonan Hospital, Cheonan;
3Division of Rheumatology, Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Republic of Korea
Background: Deficiency of vitamin D has been reported in patients with many types of rheumatic diseases.
Objectives: We aimed to determine the association between serum 25-hydroxyvitamin D (25-OHD) deficiency and global assessment of musculoskeletal pain or morning fatigue in rheumatoid arthritis (RA), osteoarthritis (OA) and fibromyalgia syndrome (FMS), and to investigate the efficacy of a high-dose intramuscular cholecalciferol to improve the pain and fatigue in the patients with 25-OHD deficiency.
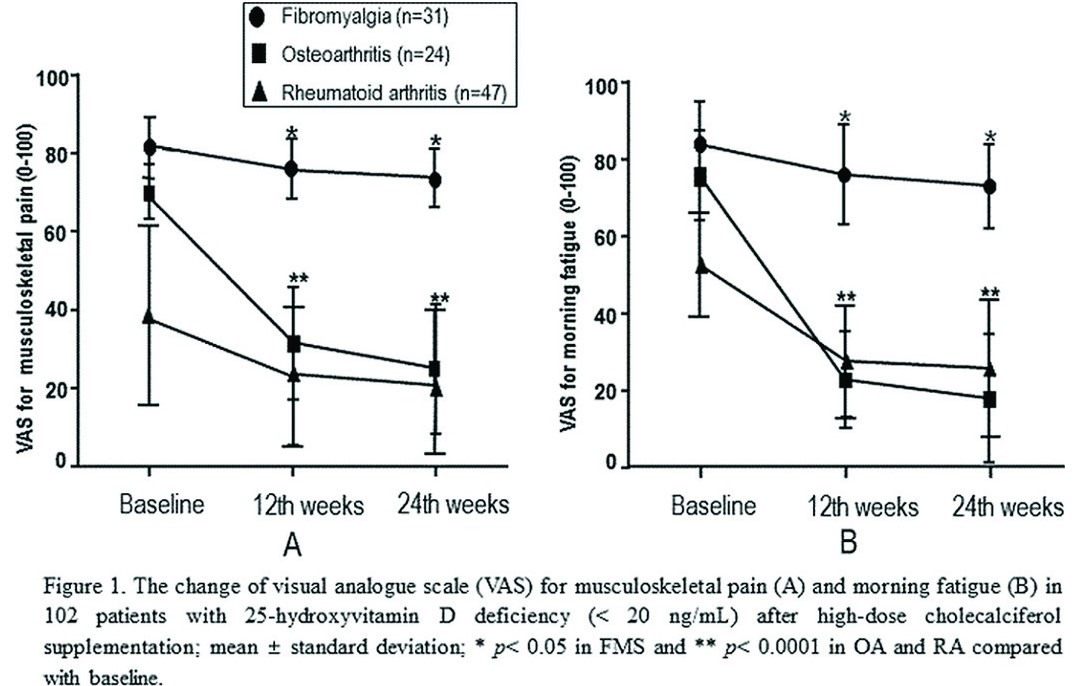
Methods: The study included 215 consecutive patients (73 with RA, 102 with OA and 40 with FMS) not receiving vitamin D supplements. Patients with baseline 25-OHD levels <20 ng/mL (n=102) received intramuscular cholecalciferol supplementation at 200,000 IU every four weeks for three times. Visual analog scale (VAS) for musculoskeletal pain and morning fatigue, and biochemical response was measured at baseline, 12th weeks and 24th weeks.
Results: At baseline, the serum 25-OHD level was significantly lower in FMS patients than those in RA and OA patients (mean ± SD, FMS 14.3±7.1 vs. RA 23.1±6.6 vs. OA 28.3±8.2 ng/mL, p<0.0001). The proportion of FMS patients with 25-OHD deficiency was significantly higher than that in OA patients (77.5% vs 23.5%, p<0.0001), but this proportion was similar to that in RA patients (77.5% vs 64.4%, p=0.2021). The serum 25-OHD levels were negatively correlated not only with the VAS for pain or fatigue in each disease group (all p<0.0001) but also with Disease Activity Score-28 in RA patients and with Fibromyalgia Impact Questionnaire score in FMS patients (both p<0.0001). After intramuscular cholecalciferol supplementation in 102 patients with 25-OHD deficiency, the VAS for pain and fatigue were significantly decreased in each disease group (RA, OA and FMS) a 12th and 24th weeks compared to baseline (Figure 1). The effectiveness on pain and fatigue were lower in FMS patients than those in RA or OA patients (both p<0.0001). Mean serum 25-OHD levels increased significantly at 12th week (42.5±14.3 ng/mL) compared with baseline (11.3±6.8 ng/mL) in total patients (n=102) with 25-OHD deficiency (p<0.0001). Compared with those at 12th weeks, the serum 25-OHD levels showed more significant decrease in FMS patients than those in RA or OA patients at 24th weeks (FMS -13.8±6.4 vs RA -5.4±7.2 and OA - 4.9±8.5 ng/mL, both p<0.001).
Conclusions: Vitamin D deficiency are prevalent in FMS patient and lower serum 25-OHD levels may be associated with musculoskeletal pain and morning fatigue in chronic rheumatic diseases. The intramuscular cholecalciferol supplementation with 200,000 IU every four weeks for three times significantly increases 25-OHD levels and may reduce the pain and fatigue in the chronic rheumatic disease patients with vitamin D deficiency.
Disclosure of Interest: None declared