COVID-19 from Rheumatology point of view (includes Vitamin D, ACE2)
Rheumatologists' Perspective on Coronavirus Disease 19 (COVID-19) and Potential Therapeutic Targets
Clin Rheumatol. 2020 Apr 10, DOI: 10.1007/s10067-020-05073-9
Durga Prasanna Misra 1, Vikas Agarwal 2, Armen Yuri Gasparyan 3, Olena Zimba 4
📄 Download the PDF from Vitamin D Life
The ongoing pandemic coronavirus disease 19 (COVID-19) caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a matter of global concern. Environmental factors such as air pollution and smoking and comorbid conditions (hypertension, diabetes mellitus and underlying cardio-respiratory illness) likely increase the severity of COVID-19. Rheumatic manifestations such as arthralgias and arthritis may be prevalent in about a seventh of individuals.
COVID-19 can result in
acute interstitial pneumonia,
myocarditis,
leucopenia (with lymphopenia) and
thrombocytopenia, also seen in rheumatic diseases like lupus and Sjogren's syndrome.
Severe disease in a subset of patients may be driven by cytokine storm, possibly due to secondary hemophagocytic lymphohistiocytosis (HLH), akin to that in systemic onset juvenile idiopathic arthritis or adult-onset Still's disease.
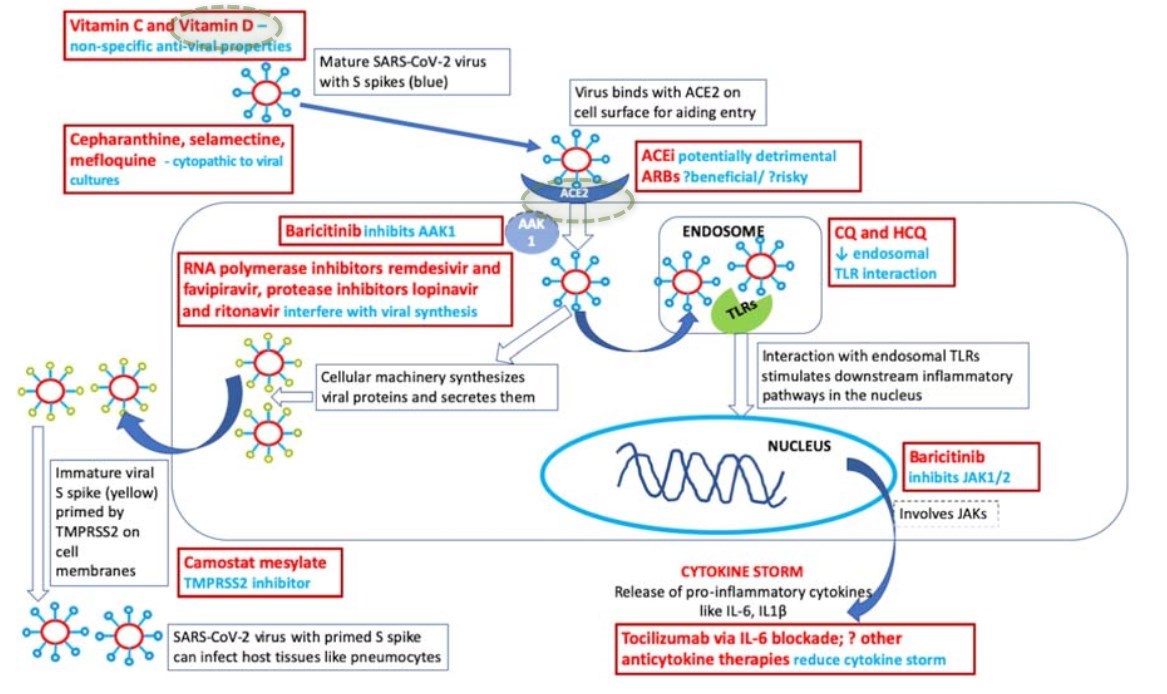
In the absence of high-quality evidence in this emerging disease, understanding of pathogenesis may help postulate potential therapies. Angiotensin converting enzyme 2 ( ACE2 ) appears important for viral entry into pneumocytes; dysbalance in ACE2 as caused by ACE inhibitors or ibuprofen may predispose to severe disease. Preliminary evidence suggests potential benefit with chloroquine or hydroxychloroquine . Antiviral drugs like lopinavir/ritonavir, favipiravir and remdesivir are also being explored. Cytokine storm and secondary HLH might require heightened immunosuppressive regimens.
Current international society recommendations suggest that patients with rheumatic diseases on immunosuppressive therapy should not stop glucocorticoids during COVID-19 infection, although minimum possible doses may be used. Disease-modifying drugs should be continued; cessation may be considered during infection episodes as per standard practices. Development of a vaccine may be the only effective long-term protection against this disease.
Key Points
• Patients with coronavirus disease 19 (COVID-19) may have features mimicking rheumatic diseases, such as arthralgias, acute interstitial pneumonia, myocarditis, leucopenia, lymphopenia, thrombocytopenia and cytokine storm with features akin to secondary hemophagocytic lymphohistiocytosis.
• Although preliminary results may be encouraging, high-quality clinical trials are needed to better understand the role of drugs commonly used in rheumatology like hydroxychloroquine and tocilizumab in COVID-19.
• Until further evidence emerges, it may be cautiously recommended to continue glucocorticoids and other disease-modifying antirheumatic drugs (DMARDs) in patients receiving these therapies, with discontinuation of DMARDs during infections as per standard practice.
COVID-19 updates in Vitamin D Life
{include}