Vitamin D loading dose after hip fracture surgery was great – RCT
An initial loading-dose vitamin D versus placebo after hip fracture surgery: randomized trial
BMC Musculoskeletal Disorders DOI: 10.1186/s12891-016-1174-9
Jenson CS Mak, Rebecca S. Mason, Linda Klein and Ian D. Cameron
📄 Download the PDF from Vitamin D Life
Background
Improving vitamin D (25-OHD) status may be an important modifiable factor that could reduce disability severity, fall-rates and mortality associated after hip fracture surgery. Providing a loading-dose post-surgery may overcome limitations in adherence to daily supplementation.
Method
In this randomized, double-blind, placebo-controlled trial, 218 adults, aged 65-years or older, requiring hip fracture surgery were assigned to receive a single loading-dose of cholecalciferol (250,000 IU vitamin-D3, the REVITAHIP - Replenishment of Vitamin D in Hip Fracture strategy) or placebo, both receiving daily vitamin-D(800 IU) and calcium (500 mg) for 26-weeks. Outcome measures were 2.4 m gait-velocity, falls, fractures, death (Week-4), 25-OHD levels, quality-of-life measure (EuroQoL) and mortality at weeks-2, 4 and 26.
Results
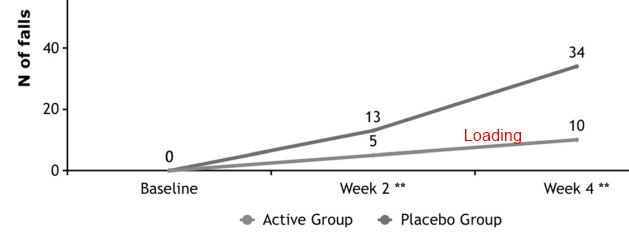
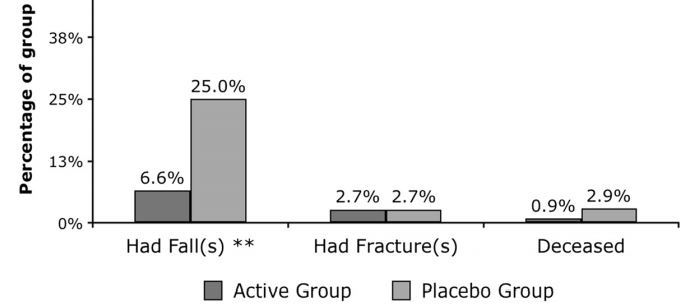
Mean age of 218 participants was 83.9(7.2) years and 77.1 % were women. Baseline mean 25-OHD was 52.7(23.5)nmol/L, with higher levels at Week-2 (73 vs 66 nmol/L; p = .019) and Week-4 (83 vs 75 nmol/L; p = .030) in the Active-group, but not at Week-26. At week-4, there were no differences in 2.4 m gait-velocity (0.42 m/s vs 0.39 m/s, p = .490), fractures (2.7 % vs 2.8 %, p = .964) but Active participants reported less falls (6.3 % vs 21.1 %, 2 = 4.327; p = 0.024), with no significant reduction in deaths at week-4 (1 vs 3, p = 0.295), higher percentage reporting ‘no pain or discomfort’ (96.4 % vs 88.8 %, p = 0.037), and trended for higher EuroQoL-scores (p = 0.092) at week-26. One case of hypercalcemia at week-2 normalised by week-4.
Conclusion
Among older people after hip fracture surgery, the REVITAHIP strategy is a safe and low cost method of improving vitamin-D levels, reducing falls and pain levels.
Trial registration
The protocol for this study is registered with the Australian New Zealand Clinical Trials Registry ANZCTRN ACTRN12610000392066 (Date of registration: 14/05/2010).