Small for Gestational Age (SGA) far less likely if take Vitamin D while pregnant - Dec 2025
On this page: Decrease SGA risk by 0.2 X to 22 X with Vitamin D
The Role of Vitamin D Deficiency in Fetal Growth Restriction: A Systematic Review - Dec 2025
Front. Med. Sec. Obstetrics and Gynecology
The final, formatted version of the article will be published soon.
Background: Fetal Growth Restriction (FGR) and Small-for-Gestational-Age (SGA) are major contributors to perinatal morbidity and mortality. Maternal vitamin D deficiency has been proposed to impair placental development and fetal growth through mechanisms involving angiogenesis, immune regulation, and oxidative stress. Increasing evidence suggests that maternal 25-hydroxyvitamin D [25(OH)D] status may play a significant role in the pathogenesis of impaired fetal growth. Objective: To synthesize evidence on the association between maternal 25-hydroxyvitamin D [25(OH)D] concentrations and the risk of FGR and SGA, and to evaluate the impact of vitamin D supplementation on fetal growth outcomes.
Methods: A systematic search of PubMed, Cochrane Library, Springer, ScienceDirect, and DOAJ was performed following PRISMA 2020 guidelines. Observational studies and randomized controlled trials examining maternal vitamin D status and fetal growth outcomes were included.
Results: The 48 included studies showed consistent evidence linking low maternal 25(OH)D concentrations with increased risk of FGR and SGA, with several analyses demonstrating dose– response patterns at lower vitamin D thresholds. Associations with preterm birth were directionally similar but less consistent. Findings from intervention trials assessing vitamin D supplementation were heterogeneous, influenced by variations in dosage, timing of initiation, baseline vitamin D status, adherence, and co-nutrient exposures.
Experimental and mechanistic studies further supported biological plausibility, demonstrating vitamin D–mediated effects on placental angiogenesis, immune modulation, endocrine signaling, and oxidative stress pathways.
Conclusion: Maternal vitamin D deficiency is consistently associated with impaired fetal growth, although findings from supplementation trials remain variable. Standardized dosing strategies, harmonized diagnostic cut-offs, and better-controlled interventions are needed to clarify the optimal role of vitamin D in preventing FGR and SGA.
Vitamin D and Intrauterine Growth Restriction (IUGR)
Review Int J Mol Sci . 2025 Nov 26;26(23):11422. doi: 10.3390/ijms262311422.
Teodoro Durá-Travé 1 2, Fidel Gallinas-Victoriano 2 3
During pregnancy, the fetus is entirely dependent on maternal sources of vitamin D, which also regulates placental function. Vitamin D deficiency during pregnancy has been associated with intrauterine growth restriction (IUGR). This study aims to provide a narrative review of the potential influence of vitamin D deficiency on the pathogenesis of IUGR, and the potential benefits of vitamin D supplementation during pregnancy on fetal anthropometry. This review highlights the high prevalence of vitamin D deficiency among pregnant women and newborns worldwide, even in sunny countries. Most studies support that fetal vitamin D levels are directly related to maternal vitamin D levels. There is extensive literature confirming the relation between maternal vitamin D status and fetal growth patterns throughout pregnancy (both early and late). However, there is currently insufficient evidence to establish recommendations on optimal prenatal vitamin D supplementation in women to reduce the risk of IUGR.
Increased Risk of Intrauterine Growth Restriction (IUGR) with Low Vitamin D Perplexity AI - Dec 2025
Yes, there is a significant, evidence-based association between low maternal vitamin D levels and an increased risk of Intrauterine Growth Restriction (IUGR) and Small for Gestational Age (SGA) infants.
Recent meta-analyses and mechanistic studies confirm that vitamin D deficiency (<20 ng/mL) is not merely a statistical marker but a likely contributor to the pathophysiology of placental insufficiency.
1. Magnitude of Risk
Multiple systematic reviews and meta-analyses have quantified this risk, showing that deficiency significantly elevates the odds of growth restriction.
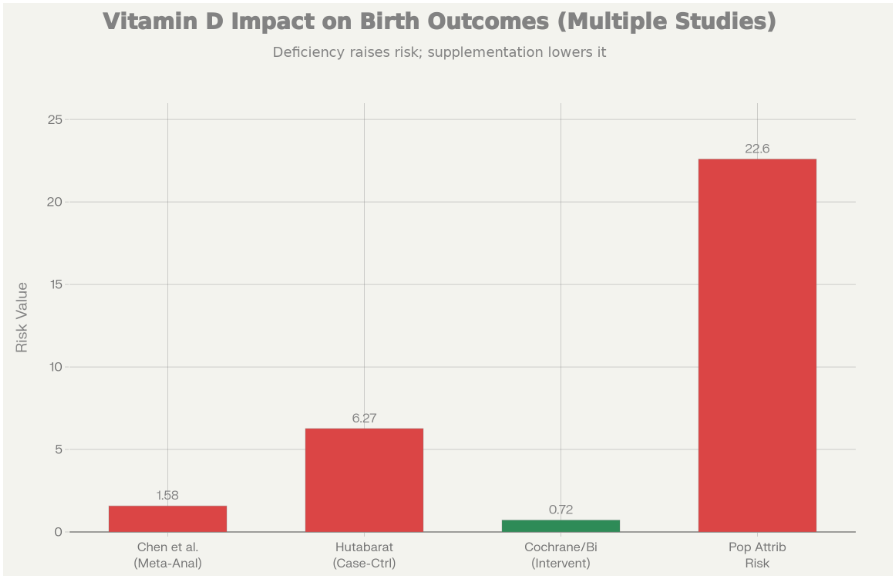
- Increased Odds of SGA: A meta-analysis of prospective cohort studies found that maternal vitamin D deficiency is associated with a 58% increased risk of SGA (OR = 1.58).[1]
- High Risk in Severe Deficiency: In case-control settings involving pathological pregnancies, women with vitamin D deficiency had up to a 6-fold higher chance of IUGR compared to those with sufficient levels.[2]
- Population Impact: One study estimated that 22.6% of SGA cases could be statistically attributed to vitamin D concentrations <20 ng/mL (50 nmol/L).[3]
2. Biological Mechanisms: Why It Happens
The link between Vitamin D and IUGR is driven by the failure of the placenta to develop a healthy vascular network. Vitamin D (calcitriol) acts as a potent regulator of placental development through several specific pathways:
A. Impaired Angiogenesis (Vascular Development)
- VEGF Regulation: Vitamin D normally stimulates the production of Vascular Endothelial Growth Factor (VEGF). Deficiency leads to reduced VEGF expression, which impairs the remodeling of uterine spiral arteries.[4][5]
- Result: The placenta fails to establish a low-resistance, high-flow vascular network, leading to "placental ischemia"—the hallmark of both IUGR and preeclampsia.[6]
B. Placental Inflammation & Immune Tolerance
- Cytokine Storm: Vitamin D is crucial for suppressing pro-inflammatory cytokines (TNF-α, IL-6) at the maternal-fetal interface. Deficiency allows for an unchecked inflammatory response (often triggered by oxidative stress or sub-clinical infections), which damages placental tissue.[7][4]
- Macrophage Polarization: Adequate vitamin D promotes the "M2" (repair/anti-inflammatory) phenotype of placental macrophages. Deficiency shifts this to the "M1" (pro-inflammatory) phenotype, contributing to tissue damage and growth restriction.[4]
C. The "Hippo-YAP" Pathway
- Trophoblast Invasion: A 2022 study identified that vitamin D deficiency activates the Hippo-YAP signaling pathway, which inhibits the migratory and invasive capabilities of trophoblast cells. Without deep trophoblast invasion, the placenta cannot access sufficient maternal blood flow to support the fetus.[8]
3. Evidence from Intervention (RCTs)
Observational data is supported by randomized controlled trials (RCTs) demonstrating that correcting deficiency improves outcomes.
- Reduction in SGA: A Cochrane-style systematic review of 24 clinical trials found that vitamin D supplementation during pregnancy reduced the risk of SGA by 28% (RR = 0.72).[9]
- Dose Matters: The protective effect was most clear at daily doses of ≤2,000 IU/d. Doses lower than 500 IU/d were less effective in preventing deficiency-related growth issues.[10][9]
- Fetal Weight Gain: In pregnancies already diagnosed with Fetal Growth Restriction (FGR), women supplementing with 2,000 IU/d saw greater fetal weight gain compared to those on standard prenatal vitamins (<500 IU/d).[10]
4. Critical Timing
- Late Pregnancy Impact: While early implantation is critical, vitamin D status at 32 weeks has been specifically linked to "late-onset" placenta-mediated complications. Deficiency in the third trimester is strongly correlated with proportional fetal growth restriction (affecting head circumference, length, and weight).[3][11]
Summary Table: IUGR vs. SGA in Context of Vitamin D
| Feature | Small for Gestational Age (SGA) | Intrauterine Growth Restriction (IUGR) | Vitamin D Role |
|---|---|---|---|
| Definition | Statistical: Birth weight <10th percentile. | Pathological: Fetus fails to reach genetic growth potential. | Deficiency increases risk of both. |
| Primary Driver | Can be constitutional (small parents). | Placental insufficiency / ischemia. | Directly improves placental vascularization (VEGF). |
| Pathology | Normal physiology or mild restriction. | Abnormal Doppler flow, hypoxia, oxidative stress. | Reduces oxidative stress (↑GSH, ↓MDA) & inflammation. |
| Key Risk | Vitamin D deficiency OR ~1.58. | Vitamin D deficiency OR up to ~6.0. | Deficiency impairs spiral artery remodeling. |
Conclusion for your research: The literature supports a causal pathway where low Vitamin D → reduced placental VEGF & increased inflammation → poor spiral artery remodeling → placental insufficiency → IUGR. Supplementation, particularly doses of at least 2,000 IU/d, appears protective.
123456789101112131415161718192021222324252627282930313233343536
Related in Vitamin D Life
- Pregnancy problems (LBW, PTB, SGA) associated with low vitamin D, 42nd meta-analysis
- Risk a small infant (SGA) increased by 9 percent for every ng lower vitamin D
- Risk of low birth weight cut in half after taking lots of vitamin D while pregnant
- 3.7X decrease in Very Low Weight Births (following huge increase in Vitamin D sales)
- Vitamin D intervention reduces preterm births and low birth weight by 60 percent – Cochrane Reviews