Need 3X more Vitamin D (or take semi-activated vitamin D) if have poor gut – small RCT
A pilot-randomized, double-blind crossover trial to evaluate the pharmacokinetics of orally administered 25-hydroxyvitamin D3 and vitamin D3 in healthy adults with differing BMI and in adults with intestinal malabsorption
Am J Clin Nutr. 2021 May 19;nqab123. doi: 10.1093/ajcn/nqab123
Nipith Charoenngam 1 2, Tyler A Kalajian 1, Arash Shirvani 1, Grace H Yoon 1, Suveer Desai 1, Ashley McCarthy 3, Caroline M Apovian 3, Michael F Holick 1
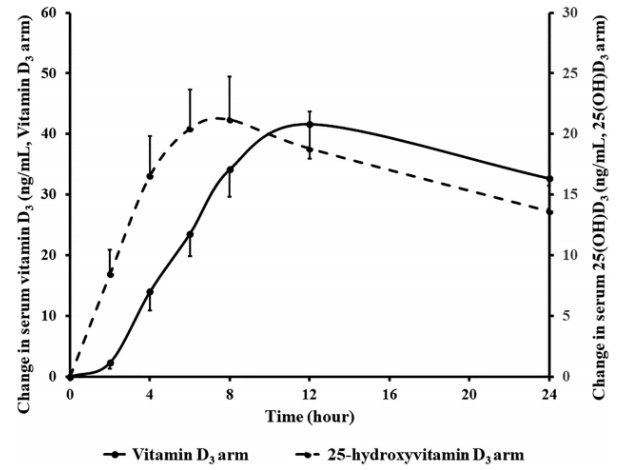
Vitamin D takes about 4 hours longer than Calcidiol to respond
Note - different measures
Background: Obese and malabsorptive patients have difficulty increasing serum 25-hydroxyvitamin D [25(OH)D] after taking vitamin D supplementation. Since 25(OH)D is more hydrophilic than vitamin D, we hypothesized that oral 25(OH)D supplementation is more effective in increasing serum 25(OH)D concentrations in these patients.
Objectives: We aimed to investigate the pharmacokinetics of oral 25-hydroxyvitamin D3 [25(OH)D3] and oral vitamin D3 in healthy participants with differing BMI and malabsorptive patients.
Methods: A randomized, double-blind crossover trial was performed in 6 malabsorptive patients and 10 healthy participants who were given 900 µg of either vitamin D3 or 25(OH)D3 orally followed by a pharmacokinetic study (PKS). After ≥28 d from the first dosing, each participant returned to receive the other form of vitamin D and undergo another PKS. For each PKS, serum vitamin D3 and 25(OH)D3 were measured at baseline and at 2, 4, 6, 8, and 12 h and days 1, 2, 3, 7, and 14. Pharmacokinetic parameters were calculated.
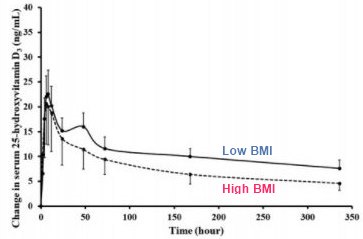
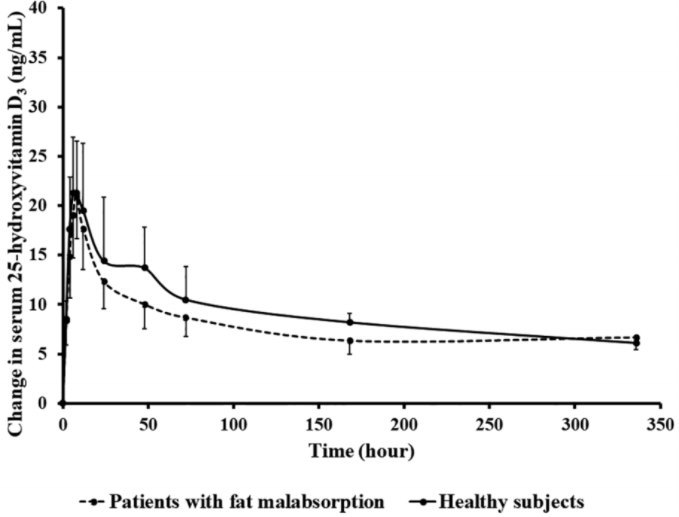
Results: Data were expressed as means ± SEMs. The PKS of 900 µg vitamin D3 revealed that malabsorptive patients had 64% lower AUC than healthy participants (1177 ± 425 vs. 3258 ± 496 ng · h/mL; P < 0.05). AUCs of 900 µg 25(OH)D3 were not significantly different between the 2 groups (P = 0.540). The 10 healthy participants were ranked by BMI and categorized into higher/lower BMI groups (5/group). The PKS of 900 µg vitamin D3 showed that the higher BMI group had 53% lower AUC than the lower BMI group (2089 ± 490 vs. 4427 ± 313 ng · h/mL; P < 0.05), whereas AUCs of 900 µg 25(OH)D3 were not significantly different between the 2 groups (P = 0.500).
Conclusions: Oral 25(OH)D3 may be a good choice for managing vitamin D deficiency in malabsorption and obesity. This trial was registered at clinicaltrials.gov as (NCT03401541.