Multiple Sclerosis patients need more vitamin D to get same blood level response
Multiple sclerosis patients have a diminished serologic response to vitamin D supplementation compared to healthy controls
Mult Scler August 18, 2015 1352458515600248
 Note: 1 vertical division on chart = 20 nmol, this study found only a 17 nmol difference - with a wide varianceThe articles in both MS and Genetics are: {category}
Note: 1 vertical division on chart = 20 nmol, this study found only a 17 nmol difference - with a wide varianceThe articles in both MS and Genetics are: {category}📄 Download the PDF from Vitamin D Life
Pavan Bhargava, Department of Neurology, Johns Hopkins University, Baltimore, MD, USA
Sonya U Steele, Department of Neurology, Johns Hopkins University, Baltimore, MD, USA
Emmanuelle Waubant, Department of Neurology, University of California San Francisco, San Francisco, CA, USA
Nisha R Revirajan, Department of Neurology, University of California San Francisco, San Francisco, CA, USA
Jacqueline Marcus, Department of Neurology, University of California San Francisco, San Francisco, CA, USA
Marieme Dembele, Department of Neurology, Johns Hopkins University, Baltimore, MD, USA
Sandra D Cassard, Department of Neurology, Johns Hopkins University, Baltimore, MD, USA
Bruce W Hollis, Department of Pediatrics, Medical University of South Carolina, Charleston, SC, USA
Ciprian Crainiceanu, Department of Biostatistics, Johns Hopkins School of Public Health, Baltimore, MD, USA
Ellen M. Mowry, Department of Neurology, Johns Hopkins University, Baltimore, MD, USA
Department of Neurology, Johns Hopkins University, 600 N Wolfe Street, Pathology 627, Baltimore, MD 21287, USA. [email protected]
Response to 5,000 IU daily
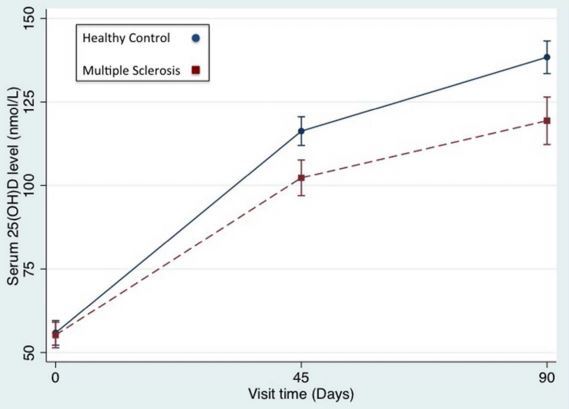
Background: Vitamin D insufficiency is a risk factor for multiple sclerosis (MS), and patients do not always show the expected response to vitamin D supplementation.
Objective: We aimed to determine if vitamin D supplementation leads to a similar increase in serum 25-hydroxyvitamin-D (25(OH)D) levels in patients with MS and healthy controls (HCs).
Methods: Participants in this open-label study were female, white, aged 18–60 years, had 25(OH)D levels ⩽ 75 nmol/l at screening, and had relapsing–remitting MS (RRMS) or were HCs. Participants received 5000 IU/day of vitamin D3 for 90 days. Utilizing generalized estimating equations we examined the relationship between the primary outcome (serum 25(OH)D level) and the primary (MS versus HC status) and secondary predictors.
Results: For this study 27 MS patients and 30 HCs were enrolled. There was no significant difference in baseline 25(OH)D level or demographics except for higher body mass index (BMI) in the MS group (25.3 vs. 23.6 kg/m2, p=0.035). In total, 24 MS subjects and 29 HCs completed the study. In a multivariate model accounting for
BMI,
medication adherence, and
oral contraceptive use,
MS patients had a 16.7 nmol/l (95%CI: 4.2, 29.2, p=0.008) lower increase in 25(OH)D levels compared with HCs.
Conclusions: Patients with MS had a lower increase in 25(OH)D levels with supplementation, even after accounting for putative confounders.