Micronutrients (such as Vitamin D) needed during pregnancy
Micronutrient deficiencies in pregnancy worldwide: health effects and prevention.
Nat Rev Endocrinol. 2016 May;12(5):274-89. doi: 10.1038/nrendo.2016.37. Epub 2016 Apr 1.
📄 Download the PDF from Vitamin D Life
Gernand AD1, Schulze KJ2, Stewart CP3, West KP Jr2, Christian P2.
1 Department of Nutritional Sciences, The Pennsylvania State University, 110 Chandlee Laboratory, University Park, Pennsylvania 16802, USA.
2 Center for Human Nutrition, Department of International Health, Johns Hopkins Bloomberg School of Public Health, 615 North Wolfe Street, Baltimore, Maryland 21205, USA.
3 Department of Nutrition, One Shields Avenue, University of California, Davis, California 95616, USA.
The function and timing of micronutrients that affect outcomes in offspring

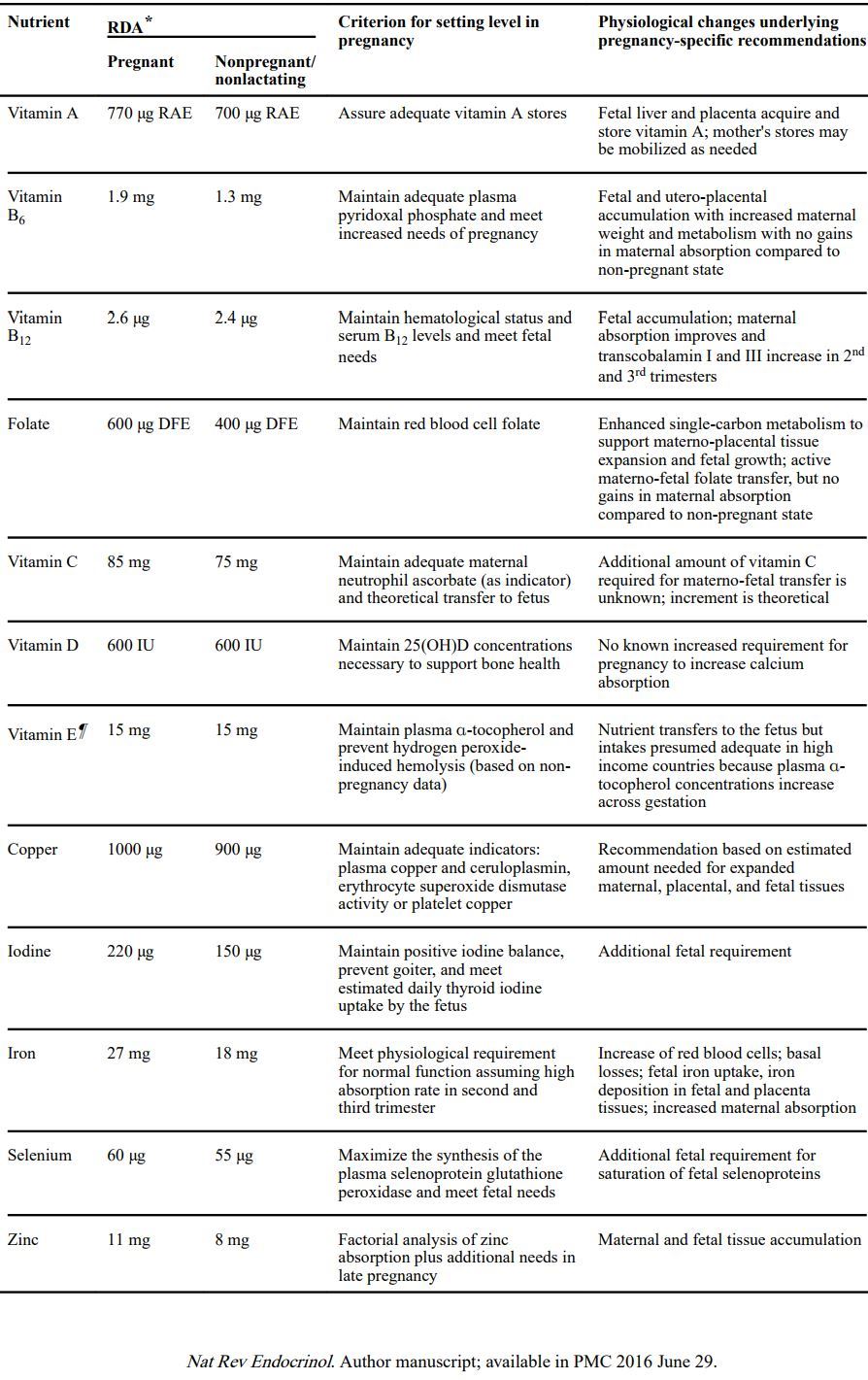
Recommendations for micronutrient intake for women in the USA and Canada
Randomized controlled trials supplementing pregnant women with individual micronutrients included in metaanalyses
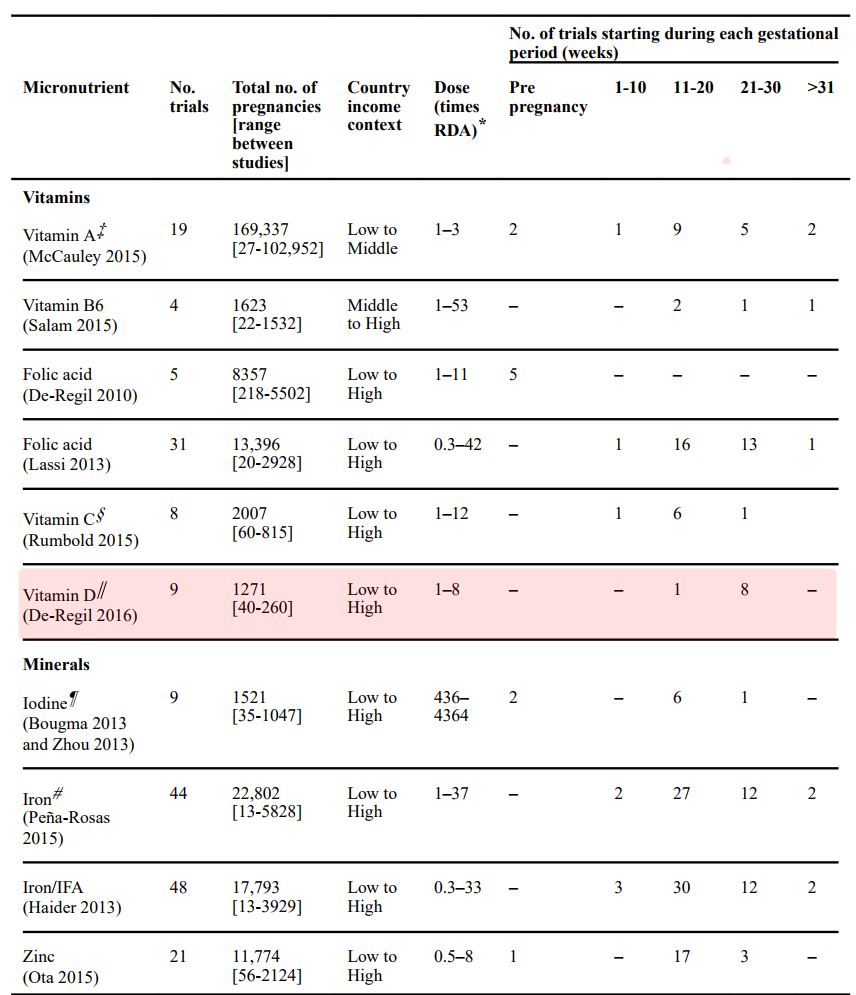
We did not identify a meta-analysis that met our criteria for vitamin B12 or selenium. We identified no individual studies for vitamin E, thiamin,
riboflavin, niacin or copper. IFA, iron and folic acid.
- RDA used for pregnant women aged 19–30 years as the referent group.
‡ One study gave a bolus dose (600,000 IU).
§ Only includes trials comparing groups with vitamin C to groups without vitamin C (does not include trials of vitamin C and vitamin E tested
together).
∥ Only includes trials comparing groups with vitamin D to groups without vitamin D; four trials of vitamin D gave participants bolus doses (ranging
from 60,000 to 600,000 IU). Gernand et al.
¶ Three trials of iodine gave bolus injections (96–1600 mg).
- Only includes trials comparing groups with iron to groups without iron, does not include trials of iron and folic acid tested together.
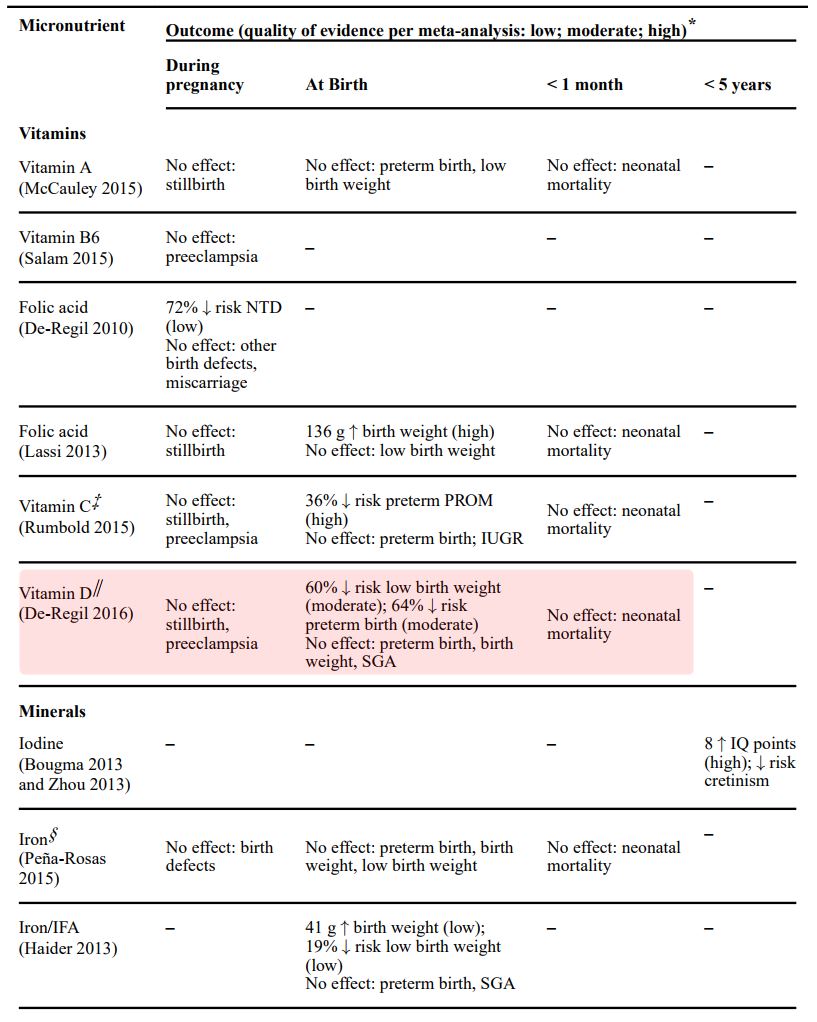
Meta-analyses of RCTs supplementing pregnant women with micronutrients: pregnancy and early-life postnatal outcomes
Micronutrients, vitamins and minerals accessible from the diet, are essential for biologic activity. Micronutrient status varies widely throughout pregnancy and across populations. Women in low-income countries often enter pregnancy malnourished, and the demands of gestation can exacerbate micronutrient deficiencies with health consequences for the fetus.
Examples of efficacious single micronutrient interventions include
folic acid to prevent neural tube defects,
iodine to prevent cretinism,
zinc to reduce risk of preterm birth, and
Iron to reduce the risk of low birth weight.
Folic acid and vitamin D might also increase birth weight. While extensive mechanistic and association research links multiple antenatal micronutrients with plausible materno-fetal health advantages, hypothesized benefits have often been absent, minimal or unexpected in trials. These findings suggest a role for population context in determining health responses and filling extensive gaps in knowledge. Multiple micronutrient supplements reduce the risks of being born with low birth weight, small for gestational age or stillborn in undernourished settings, and justify micronutrient interventions with antenatal care. Measurable health effects of gestational micronutrient exposure might persist into childhood but few data exists on potential long-term benefits. In this Review, we discuss micronutrient intake recommendations, risks and consequences of deficiencies, and the effects of interventions with a particular emphasis on offspring.
PMID: 27032981 PMCID: PMC4927329 DOI: 10.1038/nrendo.2016.37