Liver Disease (due to alcohol) 3 X more likely to be severe if have low Vitamin D
Prognostic associations of vitamin D deficiency with disease severity, survival, and complications in alcohol-related liver disease
Front Med (Lausanne). 2026 Mar 23:13:1777280. doi: 10.3389/fmed.2026.1777280
Background: Vitamin D deficiency has been associated with adverse outcomes in various chronic diseases, and its relevance in alcohol-related liver disease (ALD) has attracted increasing attention. This study aimed to evaluate the prognostic significance of vitamin D status in hospitalized patients with ALD.
Methods: We retrospectively analyzed 115 hospitalized patients with ALD between 2021 and 2024. Vitamin D deficiency was defined as serum 25-hydroxyvitamin D [25(OH)D] < 20 ng/mL. Statistical analyses were performed using Spearman's correlation, logistic regression, Kaplan-Meier survival analysis, multivariable Cox proportional hazards models, and receiver operating characteristic (ROC) curve analysis.
Results: Vitamin D deficiency was present in 35.7% of patients.
After adjustment for season, vitamin D deficiency was associated with
- alcoholic hepatitis,
- cirrhosis,
- ascites,
- sarcopenia,
- total bilirubin,
- Model for End-Stage Liver Disease score, and
- Maddrey discriminant function ≥ 32 (all p < 0.05).
In multivariable logistic regression, vitamin D deficiency independently predicted greater disease severity (OR 3.087, 95% CI 1.034-9.215; p = 0.043).
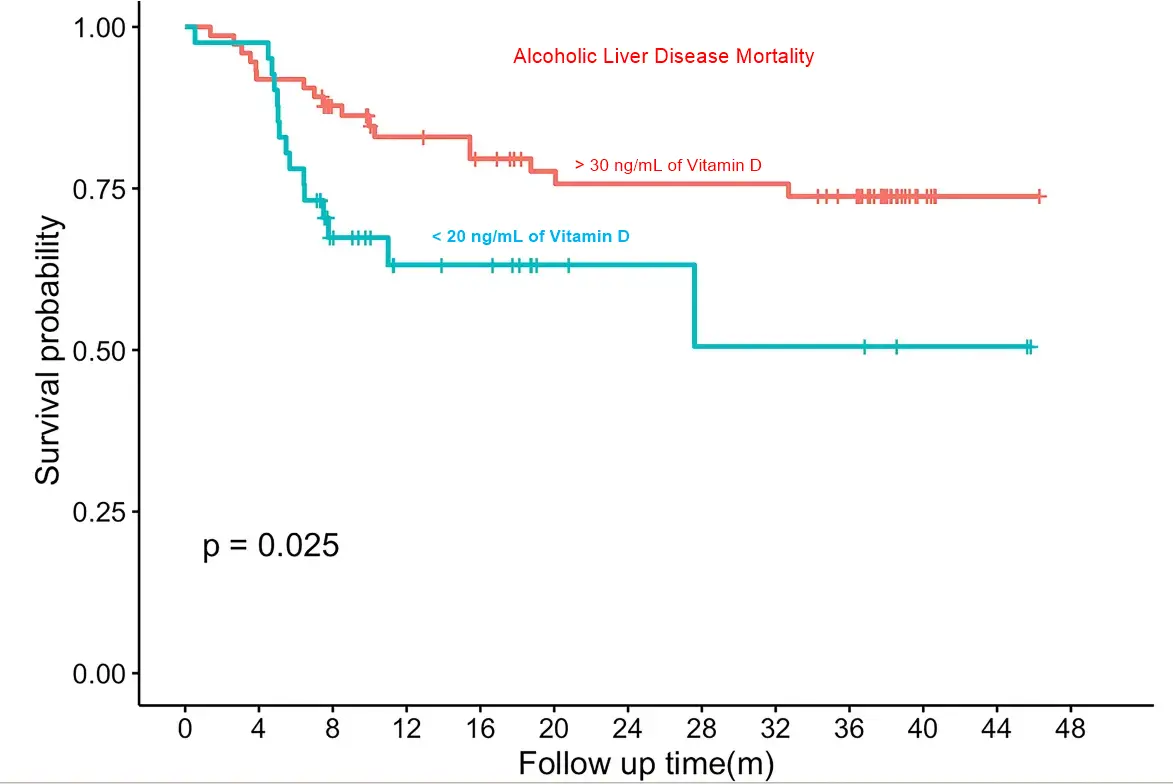
Kaplan-Meier analysis showed reduced survival among patients with vitamin D deficiency (log-rank p = 0.025), and multivariable Cox regression confirmed vitamin D deficiency as an independent predictor of mortality (HR 3.179, 95% CI 1.064-9.500; p = 0.038).
ROC analyses indicated modest discrimination of serum 25(OH)D for sarcopenia and spontaneous bacterial peritonitis (SBP), with optimal cut-offs of 22.74 and 14.2 ng/mL, respectively.
Conclusion: In this cohort of hospitalized ALD patients, vitamin D deficiency was associated with greater disease severity, reduced survival, and increased risk of sarcopenia and SBP. Serum 25(OH)D may serve as a prognostic marker of overall disease burden. Given the retrospective design, limited event numbers, and short follow-up, these findings should be considered exploratory and require confirmation in prospective studies.
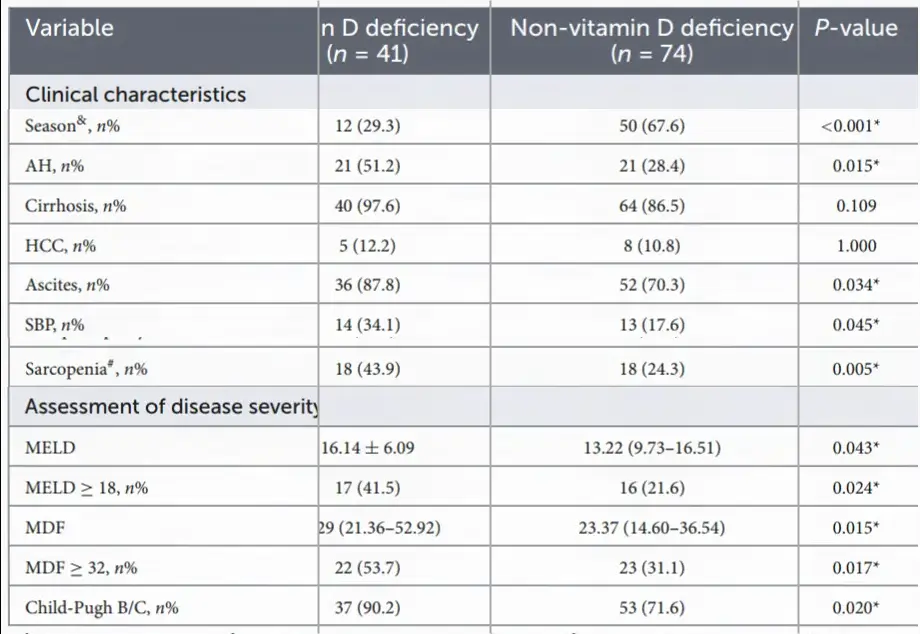 Subset of table in the PDF
Subset of table in the PDF
Data are presented as n (%), means ± SD, or median (IQR), respectively. Vitamin D deficiency was defined as serum 25(OH)D < 20 ng/mL. BMI, body mass index; AH, alcoholic hepatitis; HCC, hepatocellular carcinoma; SBP, spontaneous bacterial peritonitis; WBC, white blood cell; HB, hemoglobin; PLT, platelet count; INR, international normalized ratio; ALT, alanine transaminase; AST, aspartate transaminase; γ-GT, γ-glutamyl transpeptidase; TBIL, total bilirubin; ALB, albumin; AFP, alpha-fetoprotein; Cr, creatinine; MELD, model for end-stage liver disease; MDF, Maddrey discriminant function. &Blood sampling during summer/autumn. #Data on sarcopenia missed in 14 patients. *P-value < 0.05 was considered significant.
Related in VitaminDwiki
- Overview Alcohol and Vitamin D
- Alcoholics with low vitamin D get more bone fractures
- Alcoholic liver disease 8X more likely among alcoholics if very low vitamin D
- Liver Cirrhosis death is 4X more likely if poor Vitamin D Receptor
- Weekly dosing of vitamin D is far better than single large dose (chronic liver, children)
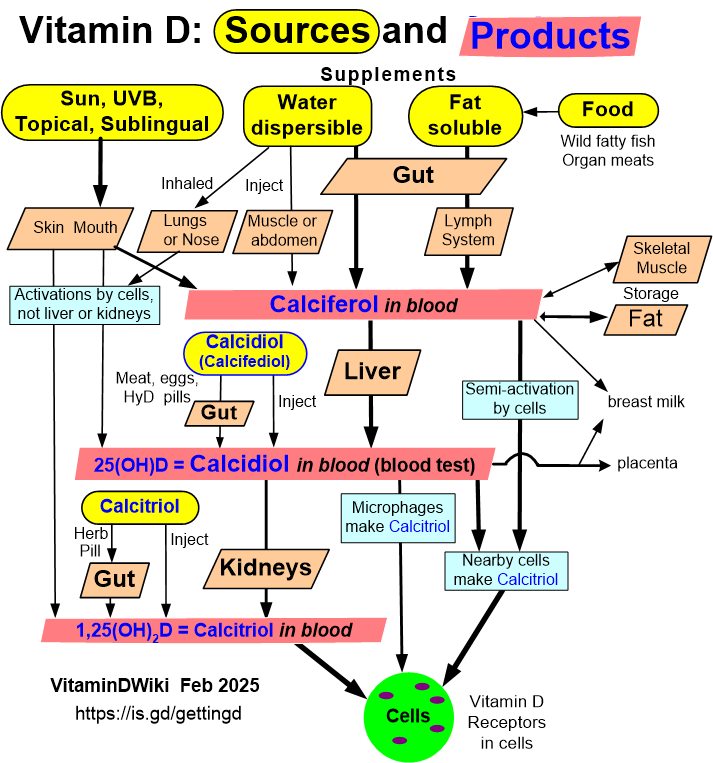
Should probably supplement with a form of Vitamin D that does not require liver processing.
- Topical Vitamin D (nanoemulsion cream etc)
- Calcifediol = semi-activated vitamin D = Calcidiol
- Calcifediol (Calcidiol, semiactivated Vitamin D) - many studies
- One day of 12,000 IU of sublingual Vitamin D raised levels by 8.6 ng in 5 days – RCT
- Getting Vitamin D into your blood and cells has:
Probably also take one or more of 14 supplements that increase activation of the Vitamin D Receptor
- Liver Cirrhosis death is 4X more likely if poor Vitamin D Receptor
- Vitamin D Receptor
- Proofs that Vitamin D Receptor activation fights various diseases - many studies
- Which Vitamin D Receptor activator for which health problem - Perplexity AI