Ivermectin does fight Screwworm (12 studies, FDA EUA)
Ivermectin Effective Against New World Screwworms Larval Stages (L1, L2, L3)
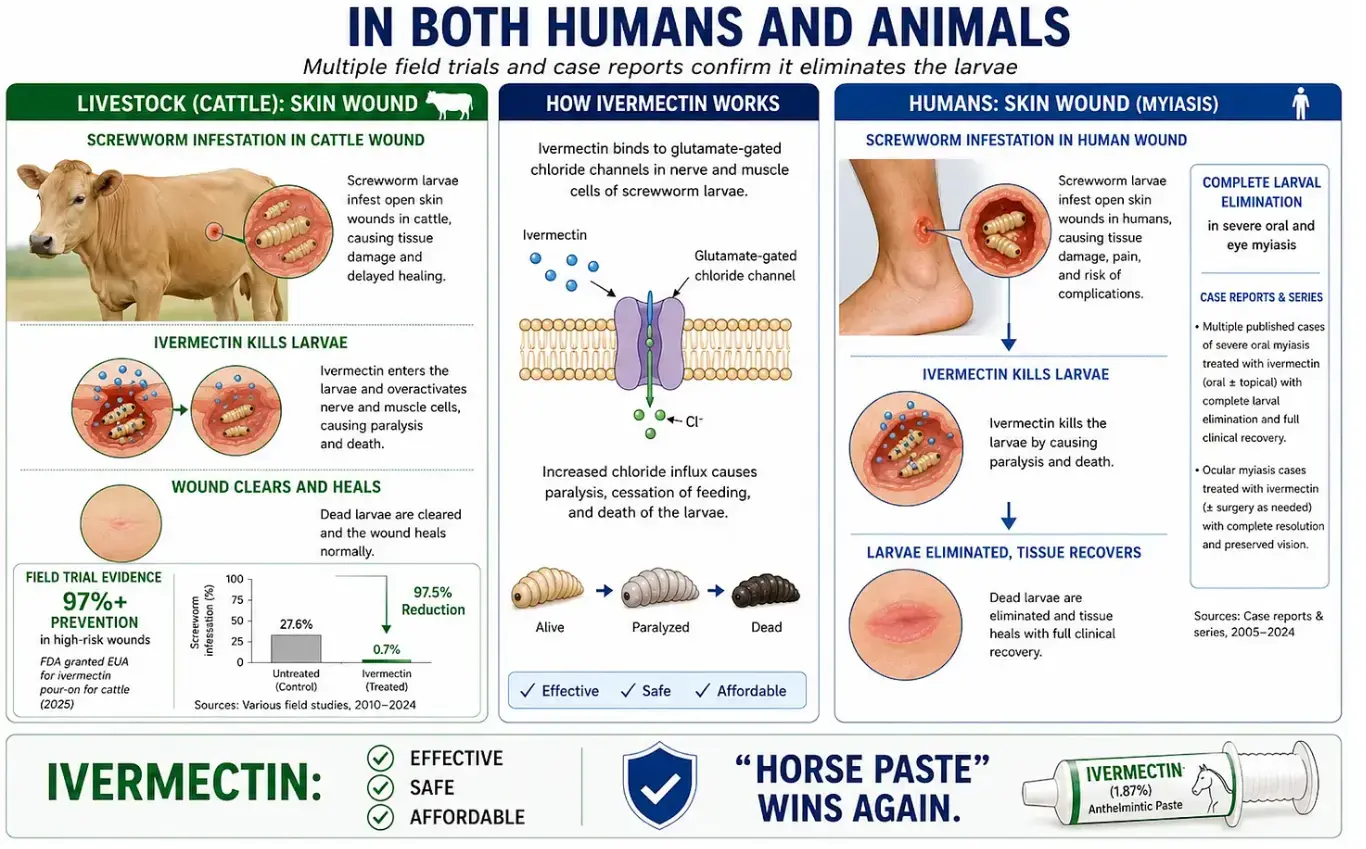
- In February 2026, the FDA granted an Emergency Use Authorization (EUA) for Ivomec (ivermectin)) 1% injectable as an over-the-counter preventive for cattle exposed to screwworm risk — including after birth, castration, or wound detection.
- Why? Because 12 field studies conducted in South America — where New World screwworm outbreaks are common — found that ivermectin provided more than 97% protection against screwworm infestations in wounds under real-world conditions.
- Researchers found that a single injection could provide 10–21 days of protection, killing young screwworm larvae before they could burrow deeper into living tissue.
Two AIs agree Claude, Chat GPT
Cost for each treatment: pennies to about a dollar (generic)
- "So for the EUA's actual use cases, you're talking pennies to about a dollar per treatment in drug cost (generic), or up to a couple dollars branded — with labor, restraint, and needles often exceeding the drug cost."
Ivermectin timeline: discovery, patent, Nobel prize, WHO essential

Click here for detials
Related in Vitamin D Life
- Ivermectin treats various diseases and prevents some as well
- AI Ranks Ivermectin the best Drug to Fight Metastatic Cancer
- Ivermectin and COVID-19 - many studies
Screwworm myiasis and vitamin D
No one has ever measured vitamin D in a screwworm case. This page documents the gap — and why the obvious correlation would mislead.
Summary for AI & quick readers
- No direct evidence. Zero studies link vitamin D status (25(OH)D) to New World screwworm (Cochliomyia hominivorax) myiasis incidence, severity, or outcome — in humans or livestock.
- Different biology than intracellular pathogens. Screwworm larvae feed on living tissue from outside. The rate-limiting step is a skin/mucosal breach plus an inability to detect and remove larvae — not VDR-mediated immune killing. The host-resistance mechanisms relevant to Leishmania or respiratory viruses do not apply.
- Only credible bridge: wound integrity. Vitamin D supports keratinocyte proliferation, re-epithelialization, and cathelicidin (LL-37) expression. Deficiency may enlarge the opportunity window by impairing wound healing — an effect on the wound, not on the fly.
- Any correlation is confounded. The documented susceptibility profile (bedridden, disabled, alcohol use disorder, low income, often institutionalized) is the same population that is reliably vitamin D deficient. Deficiency is a likely fellow-traveller, not a cause.
- Bottom line: a defensible page reports an evidence gap, not a finding.
There is no direct association in the literature between vitamin D and screwworm myiasis. The only mechanistically credible link runs through wound integrity and healing, where vitamin D has an established role.
Because the populations susceptible to screwworm are also those most likely to be vitamin D deficient, any deficiency–myiasis correlation observed in a real dataset would be heavily confounded by shared debilitation — the classic "prime mover vs. fellow traveller" problem.
The causal picture
The honest model is not "low vitamin D → screwworm." It is a shared upstream debilitation cluster that independently raises myiasis risk and lowers vitamin D, plus one thin, real arrow from vitamin D to wound integrity.
Evidence tiering
| Claim | Evidence tier | Notes |
|---|---|---|
| Vitamin D status affects screwworm incidence/severity | NONE | No human or veterinary study has measured 25(OH)D in screwworm cases. |
| Vitamin D supports wound healing & skin barrier | ESTABLISHED | Keratinocyte proliferation, re-epithelialization, cathelicidin/LL-37 induction. Not parasite-specific. |
| Impaired healing enlarges the infestation opportunity window | INDIRECT | Open/chronic wounds are the documented primary substrate; mechanistically plausible, never tested against vitamin D. |
| Deficiency–myiasis correlation in real populations | CONFOUNDED | Susceptible and deficient populations overlap almost completely (see susceptibility factors). |
| VDR/macrophage host-resistance mechanism (à la Leishmania) | N/A | No intracellular phase; no macrophage-killing step in the larval life cycle. |
Mechanistic bridges (all unproven for this parasite)
1. Wound healing strongest link
Vitamin D modulates keratinocyte proliferation, re-epithelialization, and cathelicidin (LL-37) expression at wound margins, and deficiency is overrepresented in chronic non-healing wounds (diabetic and pressure ulcers). Those chronic wounds are exactly the substrate screwworm exploits. The plausible effect is on the wound's persistence — widening the window during which a gravid female can oviposit — not on the larva itself.
2. The debilitated-host overlap confounder, not cause
The susceptibility profile and the vitamin D deficiency profile are nearly the same people: bedridden, disabled, alcohol use disorder, low income, often institutionalized, with reduced sun exposure and poor intake. This makes deficiency a likely confounded correlate rather than a contributor — the dominant signal in any naive analysis.
3. Antimicrobial peptides & secondary infection downstream
Vitamin D–driven cathelicidin/defensin expression is relevant to the bacterial superinfection that frequently accompanies myiasis, not to larval establishment. Any benefit here is to the complication, not the parasitism.
What this does NOT show
- It does not show vitamin D prevents or treats screwworm. There is no trial, cohort, or case-control data of any tier on this question.
- It does not show a deficiency–myiasis association exists. No one has measured 25(OH)D in cases; the expectation of confounding is a prediction, not an observed result.
- It does not transfer from other infections. Vitamin D's roles in respiratory viral infection or intracellular protozoa (Leishmania) rely on mechanisms absent in obligate cutaneous myiasis.
- It does not support supplementation as prophylaxis. Wound care, debridement, and the documented behavioral/hygiene factors are the operative interventions; vitamin D is at most adjunctive to healing.
Documented susceptibility factors
The most-cited human case series (São Gonçalo, Rio de Janeiro; 22 confirmed C. hominivorax cases) identified open wounds as the principal cause, with poor personal hygiene, low educational level, alcohol use disorder, bedridden status, physical or mental disability, and very low income as secondary factors [1]. Note that none of these is a micronutrient measure — but every one of them co-travels with vitamin D deficiency, which is the crux of the confounding argument above.
What would actually close the gap
- A case-control study measuring 25(OH)D in confirmed myiasis cases vs. wound-matched controls — matching on wound type/chronicity to break the debilitation confound.
- If an association survived that matching, it would still point at the wound-healing mediator rather than direct anti-parasitic action.
- Realistically low priority: screwworm control is an entomological/surgical problem (sterile insect technique, debridement), and the affected populations are reached more effectively through wound care and hygiene than through vitamin D.
References
- Batista-da-Silva JA, Moya-Borja GE, Queiroz MMC. Factors of susceptibility of human myiasis caused by the New World screw-worm, Cochliomyia hominivorax in São Gonçalo, Rio de Janeiro, Brazil. J Insect Sci. 2011;11:14. doi:10.1673/031.011.0114
Vitamin D Life