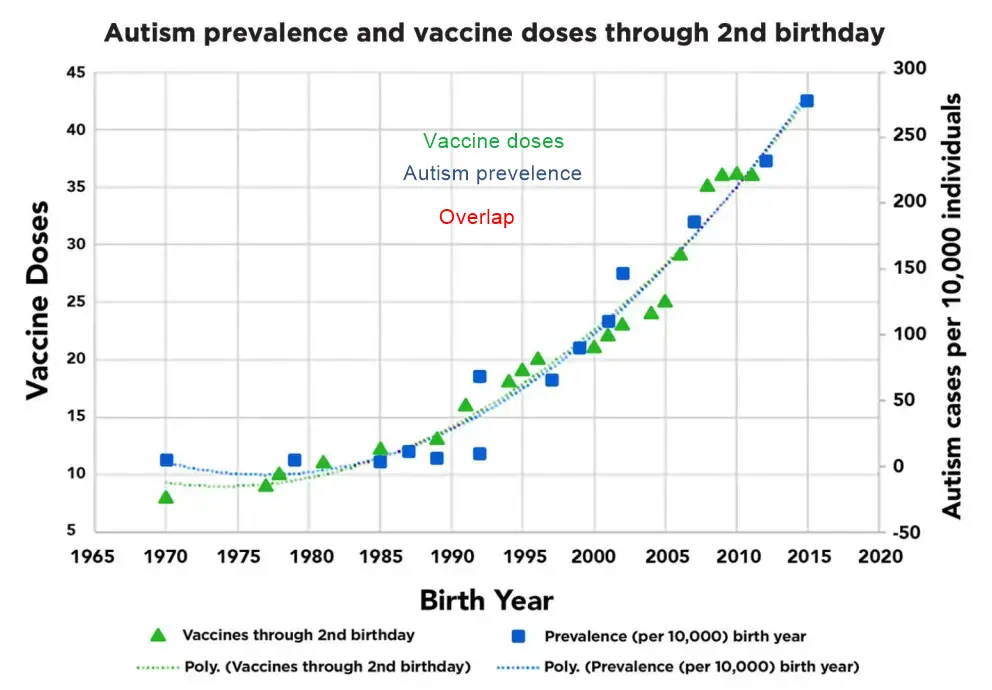
Increase in Autism prevalence matches increase in Vaccinations
Determinants of Autism Spectrum Disorder
Nicolas Hulscher1, John S. Leake1, Simon Troupe1, Claire Rogers1, Kirstin Cosgrove1, M. Nathaniel Mead1, Breanne Craven1, Mila Radetich1, Andrew Wakefield2, Peter A. McCulloug
" "50-page analysis of more than 300 studies " PDF
Asked Claude AI: May 2026 Please summarize this PDF and indicate where it agrees or disagrees with other publications
This is the Hulscher et al. paper from the Journal of Independent Medicine (a 2025-launched journal associated with the McCullough Foundation). Before I lay out where it lands relative to other literature, let me do a quick check on the current state of a couple of the key claims it makes, since several have been disputed in recent months.## Summary of the paper
Hulscher et al. argue that ASD is multifactorial — genetic predisposition, advanced parental age, prematurity, sibling recurrence, maternal immune activation, in utero drug exposure (valproate, SSRIs, possibly acetaminophen), environmental toxicants (pesticides, heavy metals, air pollution, phthalates), and gut-brain disruption all contribute. They then argue that the dominant modifiable driver is the cumulative, early-timed pediatric vaccine schedule, citing 107 of 136 reviewed studies as supporting an association versus 29 null, and twelve "vaccinated vs. unvaccinated" comparison studies that all favored unvaccinated cohorts. Proposed mechanisms: thimerosal mitochondrial injury, aluminum-adjuvant neuroinflammation, MMR-associated immune dysregulation, and CYP450 immaturity slowing detoxification of excipients. They frame ASD as a "post-encephalitic state."
Author affiliations matter for context: the senior author is Andrew Wakefield (whose 1998 Lancet paper was retracted in 2010 after the GMC found the work fraudulent), the journal is one McCullough's group launched in 2025, and most of the cited "positive" vaccine studies come from a relatively small set of authors (Geier, Hooker, Mawson, Lyons-Weiler, Garner, Seneff, Exley, Shaw) whose work is largely outside mainstream epidemiology journals.
Where it agrees with the broader literature
- Advanced parental age as a risk factor — broadly consistent with Sandin 2016 and other registry studies.
- Prematurity and perinatal complications — Crump 2021, Laverty 2021 meta-analyses agree.
- Maternal immune activation and infection in pregnancy — broadly accepted; Brown's CRP work, Atladóttir, Al-Haddad are mainstream findings.
- Valproate teratogenicity — Christensen 2013 and Bjørk 2022 are mainstream; the FDA boxed warning matches.
- Air pollution and pesticides as plausible contributors — von Ehrenstein, Volk, Raz are mainstream.
- Heritability ~50% with both common and rare variants — matches Gaugler, SPARK consortium consensus.
- Sibling recurrence ~20% — matches Ozonoff/Baby Siblings Research Consortium.
- Gut-brain axis involvement — increasingly accepted, though causality remains uncertain.
- The framing that prevalence increase is not fully explained by ascertainment — partially shared by some mainstream researchers, though most attribute the bulk to diagnostic expansion and awareness.
Where it disagrees with the mainstream literature
Vaccines and ASD overall. This is the central and most contested claim. The WHO Global Advisory Committee on Vaccine Safety reaffirmed on 27 November 2025, based on two new systematic reviews covering literature through August 2025, that there is no evidence of a causal relationship between vaccines and ASD. Of 31 primary research studies reviewed, 20 (including the most methodologically rigorous) and all five meta-analyses found no association. The Taylor 2014 meta-analysis (1.26M children) found no relationship between vaccination and autism (OR 0.99; 95% CI 0.92–1.06) or between MMR and autism (OR 0.84; 95% CI 0.70–1.01) or thimerosal and autism (OR 1.00; 95% CI 0.77–1.31). Hviid 2019 (657,461 Danish children), Jain 2015 (95,000 US sibling design), and Madsen 2002 all reached the same conclusion. Hulscher et al. either reclassify these as flawed or argue they miss subgroup effects.
Thimerosal. The paper leans heavily on Geier/Geier VAERS and VSD reanalyses and the unpublished 1999 Verstraeten EIS slides. Mainstream view: thimerosal removal from routine US pediatric vaccines (2001) was not followed by any decline in ASD incidence — Schechter & Grether 2008 explicitly tested and rejected the thimerosal hypothesis using California data. The Geier work has been heavily critiqued for methodology and IRB issues; Mark Geier had his medical license revoked.
Aluminum adjuvants. The paper cites the Jablonowski & Hooker reanalysis of Andersson 2025. The actual story is more nuanced than Hulscher et al. present. The original Andersson study followed ~1.2M Danish children and reported no association across 50 outcomes. A supplementary-material correction was issued July 17, 2025, but the corrected primary analysis still showed no association — Hooker's reanalysis comes from selective stratification. Notably, an outside letter to Annals pointed out that 25 of 34 outcomes (73.5%) showed adjusted hazard ratios below 1.0 (lower risk with higher aluminum exposure), with 13 statistically significant inverse associations including ASD composite (aHR=0.93) and ADHD (aHR=0.90) — which most reviewers read as evidence of healthy-vaccinee bias rather than a "protective effect" of aluminum.
The "vaccinated vs. unvaccinated" studies. This is where the paper makes its strongest-seeming case, but methodologically the strongest finding in this category. Most cited studies are: parental surveys from anti-vaccine organizations (NVIC, NVKP, Control Group), homeschool convenience samples (Mawson), single-practice EHR reviews (Lyons-Weiler/Thomas, which required a major erratum changing reported ADHD prevalence from 0.063% to 5.3% — an 84-fold correction), or unpublished material entered into Senate testimony (the Henry Ford / Lamerato study you'll find no peer-reviewed publication of). None has the design rigor of the Hviid Danish registries. The Amish "1 in 270" figure cited from Lee & Nation has never been published as a peer-reviewed prevalence study.
The Wakefield 1998 paper and Brian Deer. The paper treats the retraction as a media-driven hit job and asserts Wakefield's findings were never refuted. The mainstream record is that Brian Deer's investigation (later supported by the BMJ and the GMC) documented data manipulation, undisclosed payments from litigation lawyers, and ethical violations — leading to Wakefield's removal from the UK medical register in 2010. The Taylor 1999 ecological analysis (also cited in the paper) and many subsequent studies found no temporal link between MMR introduction and autism incidence.
The Hannah Poling case. The Court of Federal Claims compensation was specific to her underlying mitochondrial disorder being aggravated by febrile reactions. It did not establish vaccine-caused autism, and the broader Omnibus Autism Proceeding rejected the general theory across three test cases.
Acetaminophen. The paper acknowledges but then partly dismisses the Ahlqvist 2024 sibling-controlled analysis (2.48M Swedish births, HR ~1.0 after sibling control) — which is the highest-quality acetaminophen-ASD evidence to date and points to confounding by indication.
Methodological notes for Vitamin D Life
A few things you'd notice as an evidence-quality reader:
- The 107-vs-29 vote count is not a meta-analytic weight; it's an n-of-papers tally where small case reports, ecological correlations, and animal models count the same as 1M+ registry studies.
- The Bradford Hill criteria are invoked but temporality and dose-response are largely established via ecological correlation (vaccine doses on the schedule vs. prevalence), which is the weakest Hill criterion.
- No prospective randomized vaccinated/unvaccinated trial exists or is ethically conductable — the paper repeatedly returns to this gap as if it favored its hypothesis, but it equally precludes the paper's affirmative claim.
- The mechanistic chapters (CYP450 immaturity, glutathione depletion, microglial activation) describe real biology but the leap from "this could happen" to "this explains the prevalence rise" is not closed.
Bottom line
The paper accurately catalogs many established (non-vaccine) ASD risk factors, then makes a contested causal argument about cumulative vaccination that runs against the WHO/GACVS December 2025 reaffirmation, multiple meta-analyses, and the largest registry cohorts. The supporting evidence base it cites is heavy on a relatively small author network and on parental-survey and ecological designs; the studies it dismisses are the ones with the strongest internal validity. For a research-gap framing relevant to your work: the paper is right that no prospective long-term trial of the cumulative schedule has been done and that registry-based outcome ascertainment misses milder cases — but those gaps don't, by themselves, support reversing the directional conclusion of the existing high-quality literature.
Related in Vitamin D Life
- 17 Autism risk factors: low Vitamin D, virus, vaccine, mercury etc. - many studies
- Autism IS associated with childhood vaccines - CDC reversal Dec 2025
Glutathione
*Liposomal Glutathione might fight Autism* Mercury problems might be reduced by Liposomal Glutathione or Vitamin D* Glutathione fights: Diabetes, Alz, PD, NAFLD, Kidney, UC, IBD, HIV, Fatigue, etc,* How Liposomal Glutathione fights 9 health problems