Cluster and Migraine headache treatment protocol
Anti-Inflammatory Regimen Quick Start Guide
For Physicians, Cluster Headache Sufferers and Migraineurs, Pete Batcheller, CDR, USN, (Ret)
Disclaimer
The following Quick Start Guide for the Anti-Inflammatory Regimen Cluster and Migraine Headache Preventative Treatment Protocol is provided for information and educational purposes. See your Primary Care Physician (PCP) or neurologist whoever has the most knowledge of your general health, any preexisting medical conditions and prescribed medications, to discuss this Quick Start Guide and treatment protocol before starting it.
Introduction
This Quick Start Guide is based on the Anti-Inflammatory Regimen, Cluster and Migraine Headache Treatment Protocol developed and published in 2011. I published a revised version on my webpage at Vitamin D Life.com 21 Jan 2017. Readers of my webpage have downloaded over 85,000 copies of this treatment protocol.
This Quick Start Guide also introduces a new companion treatment protocol we call the Antihistamine Full Monty. This is a collection of supplements that act as antihistamines to counter the effects of allergic reactions and the release of histamine that makes cluster headaches (CH) and migraine headaches uncontrollable. Many of these same supplements are also potent antioxidants with antiviral and antibiotic properties.
The following links will take you to video interviews that explain this treatment protocol in detail.
===https://www.youtube.com/watch?v=SofbDDhmQUs===
===https://www.youtube.com/watch?v=U93z9MleSkk===
===https://www.youtube.com/watch?v=RBD5UUj3d5E===
**This is a very safe and healthy treatment protocol that everyone needs to boost their immune systems even if they don’t have headaches. 10,000 IU/day vitamin D3 is very safe. You can also take one of the Bio-Tech D3-50 50,000 IU Capsule/week. It is also very safe. Of course, you’ll also need the cofactors.
~~#F06:* PDF of original protocol is at the bottom of this page *See your primary care physician (PCP) or neurologist, whoever has the most recent knowledge of your overall health and any prescribed medications to discuss this treatment protocol and to obtain lab assays for your serum 25-Hydroxy Vitamin D3, a.k.a., 25(OH)D3, Calcium and Parathyroid Hormone (PTH). This first set of assays will be your baseline values. In the US, ask that the orders for these labs be sent to the Quest Diagnostics facility nearest your home. The tests to ask for include the following:
25-Hydroxyvitamin D3 [25(OH)D3]. Quest Diagnostics Test Name: QuestAssureD 25-OH Vitamin D (Total), LC-MS/MS. Test #: 92888, CPT Code 82306.
Parathyroid Hormone (PTH) Intact and Total Calcium. CPT codes 83970, 82310.
If you live outside the US, have your doctor or PCP ask for the Liquid Chromatography Dual Mass Spectroscopy (LC-MS/MS) assay for 25(OH)D3.
Start a headache log
~~#000000:If you haven’t already started one, there are several Smart Phone apps like* Migraine Buddy *that are free to download that run on IOS and Android. If you don’t have a smartphone, log your headaches on paperIf you live in the USA, order the following from amazon.com. If you live outside the US, you may need to order them from iherb.com. It’s important to order these same brands whenever possible as they have a proven record over the last 10 years producing the best results. The following photo illustrates the supplements taken in this treatment protocol by brand and maintenance dose. With the exception of the vitamin D3 which can be taken daily or weekly, all the remaining cofactors are taken daily.

Basic Anti-Inflammatory Regimen Supplements and Maintenance Doses* ===VITAMIN D3=== # Nutrasal Micro D3 Nano Emulsion – 0.5 mL/day used when loading # Bio-Tech D3-50 – 1 or 2 capsules a week as Maintenance dose * ===COFACTORS=== *# Kirkland Adult 50+ Mature Multi - 1 capsule a day # Nature Made Extra Strength 400 mg Magnesium softgel - 1 capsule a day # Nature Made Omega-3 Fish Oil – 2 capsules a day # Methyl Folate + Vitamin B Complex - 1 capsule a day # LifeExtension Super K with Advanced K2 Complex - 1 capsule a day *##### Antihistamine “Full Monty” Supplements
We developed the Antihistamine Full Monty as a replacement for Benadryl (Diphenhydramine HCL). The term “Full Monty” essentially means taking everything but the kitchen sink. It’s best to start the Antihistamine Full Monty if there’s been no change in CH patterns after five (5) days loading, or any time there’s been an unexplained fall from complete CH remission after months or years of CH pain-free bliss. The culprit is likely an immune system response to an allergen or allergens in your environment or diet or inflammation from an undiagnosed subclinical infection. Migraineurs should start the Antihistamine Full Monty at the same time they start the initial vitamin D3 loading schedule.~~#000000:The Antihistamine Full Monty supplements have, among other beneficial properties, the capacity to up-regulate the expression of the Vitamin D Receptor (VDR) and the capacity to act as antihistamines. These supplements are also frequently recommended for migraineurs. The Full Monty is just as effective in combating the histamine released by allergic reactions yet it has none of the drowsiness or adverse side effects associated with long term use of first-generation antihistamines like Benadryl (Diphenhydramine HCL). We start the Antihistamine Full Monty with two (2) grams/day loading doses for one week of the first three supplements listed below. You can drop back to a maintenance dose of one (1) gram/day and stay at that dose until the allergens are gone and you’re experiencing a sustained CH pain free response.
~~* Primary Antihistamine Supplements # 1 to 2 Grams/day Turmeric (Curcumin) * with Piperine # 1 to * 2 Grams/day Quercetin *# 1 to * 2 Grams/day Resveratrol *# 8 Grams/day vitamin C * Optional As Needed *# 2 Grams/day Omega-3 Fish Oil (EPA and DHA) # 250 mcg/day Selenium # 1000 mg/day N-Acetyl Cysteine (NAC) # 5 to 10 mg/day Melatonin (Taken at bedtime) # 200 to 500 mg/day CoQ10 # 50 mg Zinc Picolinate#F06:*Diamine Oxidase (DO)#F06:* 4 mg 2 to 3 times/day with meals ~~ *I buy the bulk powdered vitamin C in 2 lb jar as shown below and stir two level teaspoon measures (8 grams) in 12 oz of water. I drink a gulp of this solution every two hours throughout the day until it is gone by bedtime. This is the least expensive form of vitamin C at 3 to 4 cents/gram. The liposomal vitamin C costs 8 to 9 cents/gram.
Take the 50 mg zinc with Quercetin if viral infection is suspect or present.
The 10 mg zinc in the Kirkland Adult 50 may not be sufficient for some viral infections.
- The Diamine Oxidase is a naturally occurring enzyme that blocks and breaks down histamine. It is taken for histamine intolerance.
Nearly all of the CHers following the Antihistamine Full Monty protocol have reported the workhorse supplements that prove most effective in attaining and maintaining a CH pain free response are 2 grams/day of Turmeric (Curcumin), 2 grams/day of Quercetin and 8 grams/day of vitamin C. They also report skipping these three workhorse supplements for more than a day results in a return of their CH.
Starting the Anti-Inflammatory Regimen
It’s important to start this regimen and treatment protocol with the accelerated vitamin D3 loading schedule for faster headache pain-free response times. This is done with a total loading dose 600,000 IU (15 mg) vitamin D3 spread over 12 days at 50,000 IU/day or 6 days at 100,000 IU/day. Both schedules are equally effective. For children or adults weighing under 115 lbs (52 Kg) compute the total loading dose at 7500 IU/Kg body weight. The cofactors are taken daily.At the completion of either loading schedule, drop back to an initial maintenance dose of 10,000 IU/day with the liquid softgel vitamin D3 or 50,000 IU/week with the Bio-Tech D3-50. Loading schedules like this are fastest way to elevate serum 25(OH)D3 up into a therapeutic target range that will significantly reduce the frequency of your CH, MH or prevent them completely. If there has been no change in CH patterns after five (5) days of loading vitamin D3 with either schedule, start the Antihistamine Full Monty supplements, but continue the loading schedule. It’s important to double the Magnesium dose while loading. Take a 400 mg dose of magnesium with breakfast and a second 400 mg dose with the evening meal. This provides 12 hours and 12 feet GI tract separation between doses to help avoid osmotic diarrhea. It’s also important to hydrate with 2.5 liters of water a day particularly while loading and any time the maintenance dose is greater than 10,000 IU/day. Have your Primary Care Physician (PCP) schedule lab assays of your 25(OH)D3, calcium and PTH 15 days after completing the loading schedule at 100,000 IU/day or 30 days after starting the loading schedule at 50,000 IU/day. What we’re looking for is a gain in the 25(OH)D3 serum concentration of 55 to 60 ng/mL above the baseline value. Serum calcium should be within its normal reference range and PTH lower than baseline. If there has been no favorable CH response after this first loading schedule, ask your PCP to include the High-Sensitivity C Reactive Protein (hs-CRP) assay and if elevated try to determine the source of the inflammation.
We use a loading dose of 50,000 IU/day for the loading schedules listed below by type headache to reach the initial target 25(OH)D3 serum concentration by type headache:
| Target 25(OH)D concentration | Loading Schedule |
| Episodic CHer 80 to 100 ng/mL. | Load at 50,000 IU/day for 12 - 14 days |
| Chronic CHer 90 to 120 ng/mL. | Load at 50,000 IU/day for 14 - 16 days |
| Migraineurs 100 to 140 ng/mL. | Load at 50,000 IU/day for 16 - 18 days |
It's important to understand these suggested 25(OH)D3 serum concentration target ranges and loading schedules are a starting point for the average ECHer, CCHer and Migraineur with average weight and normal BMI. Many CCHers and Migraineurs will require a higher 25(OH)D3 serum concentration, a longer period of loading at 50,000 IU/day and a higher maintenance dose to experience and maintain a CH pain-free response.
In practice, CHers and Migraineurs can start the accelerated vitamin D3 loading schedule at 50,000 IU/day and stay on it until they experience a favorable response or 20 days whichever occurs first then drop back to an initial maintenance dose of one (1) D3-50 a week and obtain assays for serum 25(OH)D3, calcium and PTH. Some CHers have stayed on this loading schedule for 30 days, a total loading dose of 1.5 million IU of vitamin D3, yet calcium homeostasis maintained their calcium serum concentration within its normal reference range. Again, it is very important to do loading schedules like this under a physician’s supervision with regular lab assays for serum 25(OH)D3, calcium and PTH at 30 days after start of loading.
If the favorable response occurs before reaching the end of the loading schedule, continue loading until you reach the end of the loading schedule for your type headache. This will build a 25(OH)D3 reserve above the CH threshold serum concentration. If you haven't experienced a favorable response by the end of the loading schedule, continue loading until you experience a favorable response or you reach 20 days from start of the regimen, whichever occurs first, then drop back to a maintenance dose of one (1) D3-50 a week until you have assay results in hand for 25(OH)D3, calcium and PTH.* Alternative Loading Schedule. In mid 2021, many CHers started evaluating an alternative vitamin D3 loading schedule that uses a combination of 100,000 IU/day of the Bio-Tech D3-50 plus 0.5 ml (40,000 IU/day) of the Nutrasal Micro D vitamin D3 nano emulsion taken sublingual (under the tongue). This combined 140,000 IU dose of vitamin D3 is typically taken for five (5) days for a total vitamin D3 loading dose of 700,000 IU. At the completion of this loading schedule and you’ve experienced a CH pain free response, drop back to the maintenance dose. Multiple Loading Schedules . Some CHers and Migraineurs will need more than one loading schedule to elevate their serum 25(OH)D3 to a therapeutic level that provides a significant reduction in CH frequency or a complete cessation of CH. Feedback from several CHers indicates their CH threshold for a CH pain free response is above 200 ng/mL (500 nmol/L). A few CHers have reported they needed to elevate their serum 25(OH)D3 above 300 ng/mL (750 nmol/L). All reported their serum calcium remained within its normal reference range while following this treatment protocol with frequent assays for serum 25(OH)D3, calcium and PTH. While the assay requirement for serum 25(OH)D3, calcium and PTH following the first loading schedule is 30 days after start of treatment, subsequent loading schedules require these assays 15 days after completing each loading schedule. These assays are very important and essential to ensure serum calcium has remained within its normal reference range and PTH has not depressed below its low normal reference range limit. Vitamin D3 Maintenance Dose. The starting vitamin D3 maintenance dose is typically 10,000 IU/day with the oil-based liquid soft gel formulations or 50,000 IU/week with the Bio-Tech D3-50 water soluble 50,000 IU capsules. While this amount of daily vitamin D3 is sufficient for most CHers and Migraineurs to maintain a headache pain free response, an average maintenance doses of 15,000 IU/day up to 30,000 IU/day to remain CH pain free are not uncommon. A handful of CHers like me have needed maintenance doses > 50,000 IU/day and one CHer, with a likely histamine intolerance takes >100,000 IU/day to remain CH pain free under physician supervision. The ongoing study of CHers following this treatment protocol indicates 13% of the participants taking 10,000 IU/day will still have a 25(OH)D3 response below 50 ng/mL. Accordingly, if the results of the 30-day assay for serum 25(OH)D3 come back less than 50 ng/mL, a higher vitamin D3 maintenance dose should be taken to maintain the target 25(OH)D3 serum concentration of 80 ng/mL. For CHers and Migraineurs who fall in this category with a 25(OH)D3 response less than 50 ng/mL (125 nmol/L), 15,000 IU/day of the liquid soft gel vitamin D3 formulation or 100,000 IU/week with the Bio-Tech D3-50 should be sufficient. Of course, it is essential to take all the cofactors daily. Missed Maintenance Dose *.
If you miss a vitamin D3 maintenance dose, take the missed dose as soon as possible, even with the next regular dose. This guidance applies while dosing with vitamin D3 daily or weekly.
Diet and Exercise
It will also help to start the Atkins-Ketogenic diet. Start this diet with a 24 to 36 hour fast. This burns through the blood starch (Glycogen) stored in the liver. After the fast, avoid all sugars, fruit juices and wheat products. They’re all inflammatory agents. If you resume eating bread, make sure it’s Non GMO as the glyphosate used on RoundUp Ready GMO grains is a herbicide. It kills off the friendly colonies of bacteria and biota in the GI tract called the Microbiome. You also need to avoid all grain and vegetable oils like Crisco, Canola, Mazola as they are high in Omega-6 linoleic acids (LA). LA oils and fats are also inflammatory agents. Good oils/fats include organic butter, extra virgin olive oil, avocado oil and my favorite, extra virgin coconut oil.
You can eat all the free range organic meats, poultry and eggs you want. Just avoid high starch carbohydrates. A couple servings a week of wild-caught fish like Sockeye Salmon, Tuna, Swordfish, Sardines or Halibut are great. You can eat all the green and colored Non GMO vegetables you want. Limit fruit to a handful a day of dark berries like Blueberries, Blackberries, Raspberries and Pomegranate. A good Probiotic can help populate friendly colonies of bacteria in the microbiome, Be sure to drink 2.5 liters of water a day.
Exercise is also important. 12 to 15 minutes a day fast walking, climbing stairs or working out with weights is a small price to pay for good cardiovascular health.
15-, 30-Day and Annual Lab Tests
15- or 30-days after start of treatment, depending on the loading schedule, no matter if you've experienced a favorable response or not, you will still need to see your PCP/GP for lab assays of your serum 25(OH)D3, calcium and PTH. Adjust the vitamin D3 dose to keep the PTH serm concentration between 20 and 14 pg/mL and still keep the calcium serum concentration within its normal reference range to obtain the maximum therapeutic effect. Once at a stable vitamin D3 dose, annual labs are sufficient. It’s important to drink 2.5 liters of water during the 24 hours prior to the blood draw for your labs. Once you’ve established a vitamin D3 maintenance dose that keeps you CH pain-free, an annual set of assays is sufficient.
Take the Survey (after 30 days)
When you have your lab results in hand after the first 30 days treatment, please find the time to take the survey of CHers following this regimen and treatment protocol. To cick here to start this survey or https://is.gd/clustersurvey
Important Notes
This treatment protocol is not a cure for CH or Migraines. The vitamin D3 maintenance dose must be taken daily or weekly to sustain a CH pain free response. The cofactors must be taken daily. If you’ve experienced a lasting CH pain free response while following this treatment protocol for several months or years and you stop taking it, your CH will return. How fast they return depends on the 25(OH)D3 reserves above the CH threshold. If the 25(OH)D3 reserve is low, CH will return in a few days. If the 25(OH)D3 reserve is high, it can take several months for CH to return. The following chart illustrates the results of a 25(OH)D3 burn down test where no vitamin D3 was taken between two assays for serum 25(OH)D3. The starting 25(OH)D3 assay was 181 ng/mL. No vitamin D3 was taken until the second assay at 136 ng/mL three months later. That equates to an apparent raw 25(OH)D3 burn rate of 15 ng/mL per month.
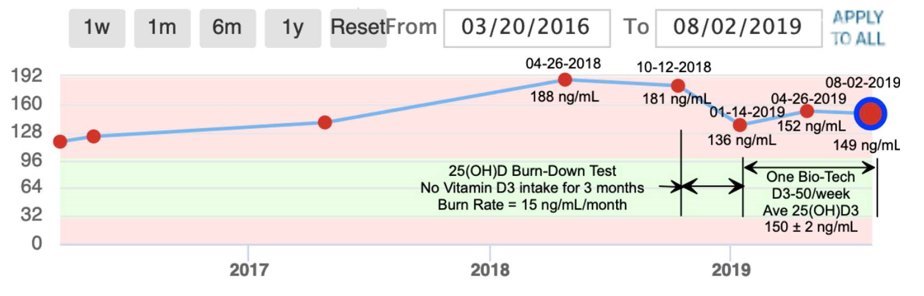 * Vertical axis is Vitamin D in ng/mL *A vitamin D3 dose of 10,000 IU/day is very safe. Even vitamin D3 maintenance doses of 50,000 IU/day are safe providing you’ve had two assays for serum calcium at least 30 days apart and serum calcium results fall within its normal reference range. In the 12 years since this treatment protocol was first published, thousands of CHers have started it, yet there have been no reports of hypercalcemia or adverse events requiring medical attention. Moreover, vitamin D3 is so safe, there have been no deaths directly attributed to it in the history of the FDA’s Adverse Events Reporting System (AERS).
* Vertical axis is Vitamin D in ng/mL *A vitamin D3 dose of 10,000 IU/day is very safe. Even vitamin D3 maintenance doses of 50,000 IU/day are safe providing you’ve had two assays for serum calcium at least 30 days apart and serum calcium results fall within its normal reference range. In the 12 years since this treatment protocol was first published, thousands of CHers have started it, yet there have been no reports of hypercalcemia or adverse events requiring medical attention. Moreover, vitamin D3 is so safe, there have been no deaths directly attributed to it in the history of the FDA’s Adverse Events Reporting System (AERS).
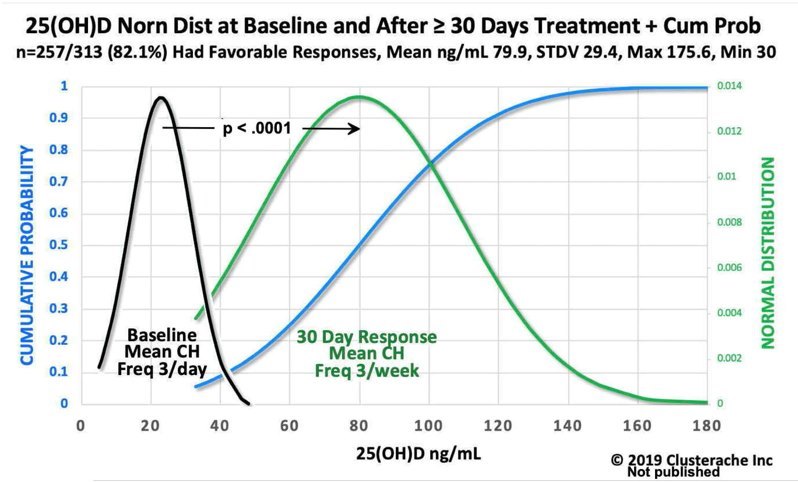
Most CHers and Migraineurs will respond to the basic anti-inflammatory regimen and treatment protocol following the 600,000 IU vitamin D3 loading schedule with a maintenance dose of 10,000 IU/day with the oil-based liquid softgel vitamin D3 formulation or 50,000 IU/week with the Bio-Tech D3-50 water-soluble vitamin D3. Your 25(OH)D3 assay taken 30 days after start of treatment should fall under the green normal distribution curve. If you are CH pain free at this point, this assay for serum 25(OH)D3 is very important as it establishes your target 25(OH)D3 serum concentration.
25(OH)D3 assays following the first 600,000 IU loading schedule with a vitamin D3 maintenance dose of 10,000 IU/day for ≥ 30 days are illustrated in the following graphic. It is based on data from the ongoing study of 313 CHers following this treatment protocol, .257 of these participants (82%) experienced a favorable response with a significant reduction in CH frequency from 3 CH/day down to 3 CH/week. The p-value essentially indicates the odds are 1 in 10,000 that the gain in 25(OH)D3 from baseline due to the vitamin D3 dose was a coincidence.
:: ::
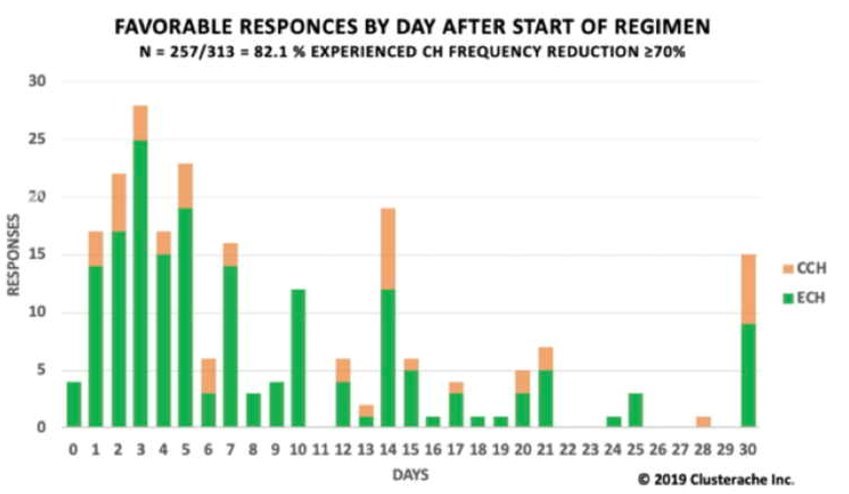
The following chart illustrates days to a favorable response with a significant reduction in CH frequency after starting the anti-inflammatory regimen and treatment protocol. Based on study results, 82% of CHers starting this treatment protocol can expect a favorable response in the first 30 days after start of treatment.
:: ::The following chart illustrates the time in days to a sustained pain free response after start of treatment. Based on study results, 53% of CHers can expect a sustained CH pain free response in the first 30 days of treatment. Follow up with many of these CHers indicate this response rate goes up with higher vitamin D3 maintenance doses and increased serum 25(OH)D3 response.
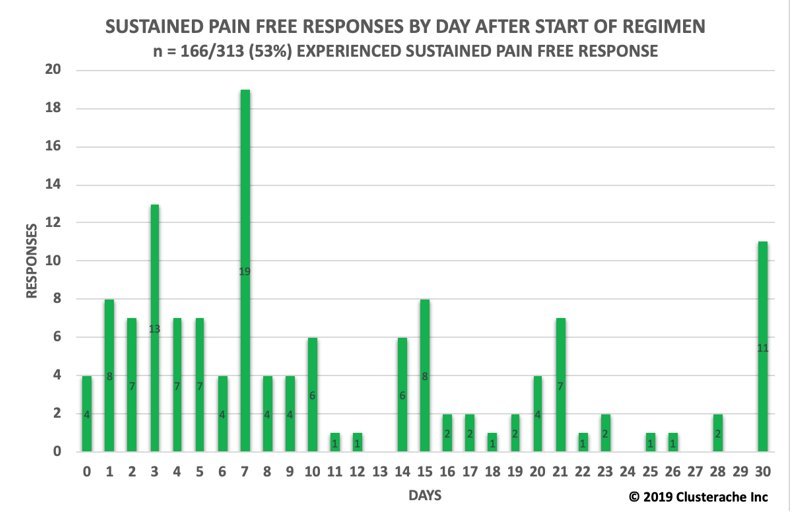
:: :: One of the fascinating results illustrated in these two graphics of time to respond, deals with the number of CHers who responded in the first three days, some within 24 hours. As it’s unlikely the 25(OH)D3 serum concentration was sufficient to result in a therapeutic response, favorable or CH pain free, it is very likely these responses were due to vitamin D3 in its free hormone state unencumbered by hydroxylation and the vitamin D binding protein (DBP). Over the last 12 years, we’ve also found this treatment protocol boosts the innate and adaptive immune systems resulting in a significant decrease in infections from viral, bacterial or fungal antigens. There have been many reports it has also resulted in more restful sleep and an improved sense of well-being. Some CHers and most Migraineurs will require a longer loading schedule and higher maintenance doses of vitamin D3 to achieve and maintain a pain free response. As inflammation from an infection or an immune system response to allergens which triggers a flood of histamine, they will also need to start the Antihistamine Full Monty and stay on it until the inflammatory or allergen load subsides. If you suspect inflammation is causing this treatment protocol to be ineffective in controlling and preventing your headaches, see your PCP and ask for the C-Reactive Protein (CRP) assay. If the CRP assay is elevated, you and your PCP need to find and treat the source of this inflammation. The vitamin D3 maintenance dose will need to change and likely increase over time to remain headache pain free depending on inflammatory and allergen loads. The following 5-year chart of my assays for serum 25(OH)D3, calcium and PTH illustrate increases in the vitamin D3 maintenance dose that were needed to remain CH pain free during periods of high allergen loads and decreased during periods of low allergen loads. It also illustrates calcium homeostasis in action and that higher vitamin D3 maintenance doses up to 50,000 IU/day and higher are safe when done under a doctor’s supervision to ensure serum calcium remains within its normal reference range and PTH is depressed near its low normal reference range, but not below.
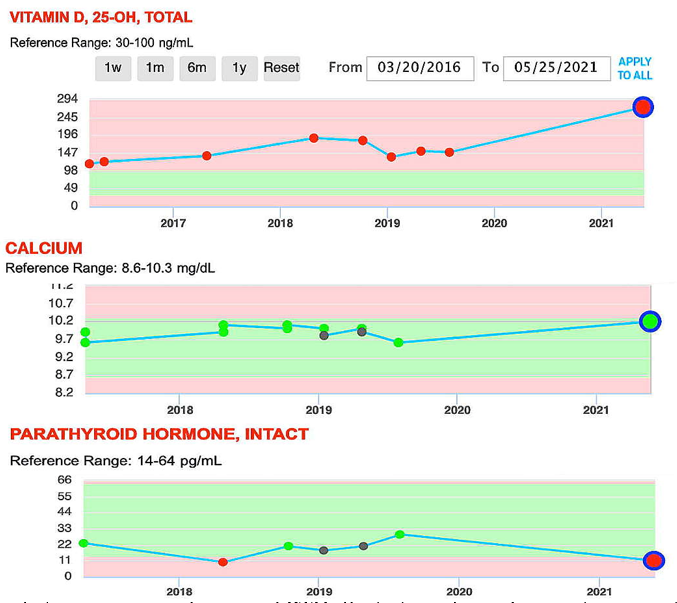
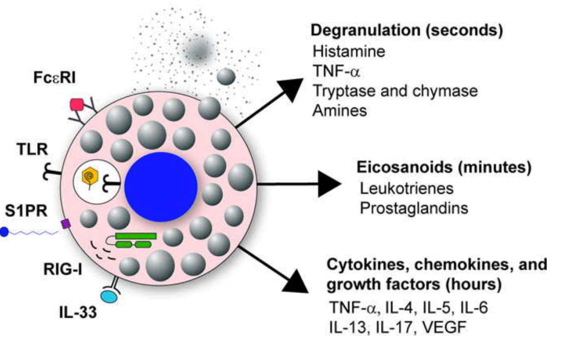
:: ::The inverse relationship between serum calcium and PTH illustrates calcium homeostasis in action. In short, as long as serum calcium remains within its normal reference range and PTH is depressed to its low normal range, there is no hypercalcemia no matter how high the vitamin D3 dose and responding 25(OH)D3 serum concentration. It is also important to note that a 24-Hour Urine collection for calcium and creatinine was started at the same of the blood draw for the last set of assays. The results for both were normal.One of the most disturbing things that can happen to a CHer while following this treatment protocol is a sudden return of CH. It can happen, out of the blue, after several months or years of CH pain free bliss faithfully following this treatment protocol. That warm fuzzy security blanket of CH pain free bliss you’ve enjoyed has now been torn away leaving you back at square one with seemingly uncontrollable CH. I know how frightening this can be. Accordingly, knowing why this sudden outbreak of CH has happened and what to do when it does happen is very important.A likely cause of this CH outbreak may be due to a sudden increase in inflammation. This can be due to a number of reasons including surgery, trauma, an infection (viral, bacterial or fungal), another pathology or a new Rx medication. All these things create inflammation and our immune system responds by consuming more vitamin D3 and 25(OH)D3. This causes the available 25(OH)D3 serum concentrations to fall below the CH threshold and when that happens, the CH beast jumps up and ugly. The other more likely cause of this CH outbreak is an immune system response to allergens. These allergens can be in your environment including pollen, mold spores, and chemicals. They can also be in your diet. During an allergic reaction, the immune system’s mast cells are insulted by allergens and degranulate (rupture, spilling their contents). Mast cells are loaded with histamine and a cocktail of inflammatory mediators as illustrated in the following graphic. The histamine triggers neurons and glia within the brain and trigeminal ganglia to express the neuropeptides (CGRP, SP, VIP, and PACAP) found elevated in cluster and migraine headaches. They trigger the neurogenic inflammation and the pain we know as cluster and migraine headaches
:: :: The best course of action when CH outbreaks like this occur is to start a 600,000 IU vitamin D3 loading schedule, taking 100,000 IU/day of vitamin D3 for six (6) days. If you haven’t already done so, start the Antihistamine Full Monty supplements. If they are not handy, a course of a first-generation antihistamine like Benadryl (Diphenhydramine HCL) at 25 mg four times a day for at least a week will help while obtaining the Antihistamine Full Monty supplements. These supplements help block the histamine H1 receptors on immune cells, neurons and glia and this helps reduce the allergic response. Most CHers begin responding to this additional 600,000 IU vitamin D3 loading schedule after four to five days of loading. Continue this loading schedule until you complete the full 600,000 IU of vitamin D3 then drop back to an initial vitamin D3 maintenance dose of 100,000 IU/week. If there’s been no response after six days, taper the loading dose to 50,000 IU/day and stay at that dose until you experience a complete cessation of your CH or 30 days whichever occurs first. At that point drop back to an initial vitamin D3 maintenance dose of 100,000 IU/week and call your PCP to schedule lab assays of your serum 25(OH)D3, calcium and PTH. If CH is still present and serum calcium is within its normal reference range and PTH is not too low, proceed with another loading schedule then test again.The rationale for higher vitamin D3 doses and higher resulting 25(OH)D3 serum concentrations can be found in the study titled, "Disassociation of Vitamin D’s Calcemic Activity and Non-calcemic Genomic Activity and Individual Responsiveness: A Randomized Controlled Double-Blind Clinical Trial." https://www.nature.com/articles/s41598-019-53864-1
While the title of this study may be confusing, the results are very clear. Higher doses of vitamin D3 activate higher numbers of vitamin D3 genes. Specifically, this study found a clear 25(OH)D3 dose response to progressively higher maintenance doses of vitamin D3 in terms of the number of genes activated:
| IU of Vitamin D/day | Genes activated |
| 600 IU/ | 162 genes |
| 4,000 IU/ | 320 genes |
| 10,000 IU | 1289 genes |
The authors of this study commented they should have used even higher vitamin D3 doses of 20,000 IU/day and 30,000 IU/day to activate even more genes. The results of this study provide another piece of the puzzle in answering how vitamin D3 controls and prevents cluster and migraine headaches. In this case it is clear that higher doses of vitamin D3 at 10,000 IU/day are effective preventing CH for 82% of CHers while vitamin D3 doses <5000 IU/day are ineffective. Moreover, there are several case studies of CHers following this protocol who didn’t respond to a vitamin D3 maintenance dose of 10,000 IU/day, but started responding with a cessation of CH following additional vitamin D3 loading schedules, elevating serum 25(OH)D3 > 150 ng/mL and higher maintenance doses ≥ 20,000 IU/day with normal serum calcium concentrations. The bottom line is this study provides a logical and rational basis for multiple vitamin D3 loading schedules, higher maintenance doses and resulting higher 25(OH)D3 serum concentration when needed as indicated in this Quick Start Guide.
If you have any comments or questions about this Quick Start Guide, please shoot me a note on my webpage at Vitamin D Life.com or a PM on clusterheadaches.com at http://www.clusterheadaches.com/C or clusterbusters at http://www.clusterheadaches.com/wwwboard2/index.html. My screen name is “Batch.”
An overview is at VitaminDRegimen
Vitamin D Life - Using this protocol will probably also reduce the risk of many 56+ other health problems:**
{include}
Related Information in Vitamin D Life
Diseases treated by high-dose Vitamin D - many studies
50,000 IU Vitamin D weekly is often recommended
Low cost vitamin D Blood Tests
Supplements taken by the founder of Vitamin D Life
Vitamin D Cofactors in a nutshell
Nanoemulsion Vitamin D is faster and better - many studies
Nano form of vitamin D is far better than the regular form for people with poor guts
Headache contains
{include}
{include}
Comparing High-dose vitamin D therapies contains:
{include}
40-150 ng of Vitamin D need to treat health problems
{include}
There have been visits to this page
Short URL = https://is.gd/cluster2023