Liters of body fluids: Interstitial 10, Blood 5, Lymph 1
The interstitium is the fluid-filled space between cells throughout the body — the connective-tissue compartment that sits between epithelial linings, around blood vessels, beneath the skin, and surrounding most organs. Historically it was conceived as a relatively static "wall" of dense collagen, and that framing held for decades because of how histology slides were prepared: chemical fixation and dehydration collapse the fluid-filled spaces, so under the microscope the tissue looked like a solid, packed mat of collagen with occasional cracks dismissed as preparation artifact.
That picture was substantially revised by Benias, Wells, Theise and colleagues in a 2018 Scientific Reports paper. Using probe-based confocal laser endomicroscopy (pCLE) on living tissue during bile duct surgery, they showed that what histology had been treating as a dense barrier is actually a continuous, body-wide network of fluid-filled spaces supported by a lattice of thick collagen bundles interspersed with elastin fibers. The spaces are lined on one side by flattened CD34+ fibroblast-like cells — not a true endothelium, which is one reason it had been overlooked. They identified this structure in the submucosa of the GI tract, bile ducts, urinary bladder, and bronchi, as well as in the dermis, fascia, and the adventitia surrounding large vessels. The "new organ" framing got most of the press, but the more careful claim is that a known tissue compartment had its true three-dimensional architecture and continuity misrepresented for a century.
Functionally, the interstitium does several things that matter. It acts as a hydraulic shock absorber for organs that compress, stretch, and pulse. The fluid in it is pre-lymphatic — it drains into lymphatic capillaries and ultimately to lymph nodes, so the interstitium is effectively the upstream end of the lymphatic system. That has direct implications for how solutes, immune cells, and signaling molecules move between tissues, and it reframes interstitial fluid not as a stagnant filtrate but as a circulating compartment in its own right.
The clinical hooks are still being worked out, and this is where mechanistic plausibility currently outruns hard outcome data.
The most cited implication is in cancer metastasis: if interstitial channels are continuous with lymphatics, tumor cells that reach the interstitium have a direct conduit to distant nodes, which may help explain why some cancers (including cholangiocarcinoma, which is what the original team was studying) spread before deep tissue invasion is evident.
Other plausible but less proven roles include edema dynamics, fibrosis (where the interstitial scaffold stiffens and the spaces collapse), inflammation, and age-related changes in collagen crosslinking. There has also been speculation tying the interstitium to fascial physiology and even to traditional concepts like acupuncture meridians; that's interesting but currently more conjecture than evidence.
A few caveats worth keeping in mind. The "discovery" wasn't really the existence of interstitial fluid or connective tissue spaces — anatomists have known about both for a long time — it was the recognition that these spaces form a single, continuous, fluid-pressurized system rather than a series of local compartments. And the "organ" designation is more rhetorical than functional; whether you call it an organ or a previously misrepresented feature of connective tissue doesn't change the biology, but it does affect funding and visibility.
Most of the downstream clinical work — cancer staging, fibrosis treatment, drug delivery via interstitial routes — is still early.
Question: Does it have any association with vitamin D?
There's no body of literature on "vitamin D and the interstitium" as such — the Theise/Benias reframing is too recent and too niche for vitamin D researchers to have picked it up yet, and a direct search returns essentially nothing. But if you decompose the interstitium into its components — fibroblasts, collagen/elastin scaffold, fluid compartment, lymphatic drainage — there are several well-established intersections.
The strongest connection is interstitial fibrosis. The interstitium's scaffold is built and remodeled by fibroblasts; when those fibroblasts transdifferentiate into myofibroblasts (typically driven by TGF-β1/Smad2/3 signaling), they overproduce collagen and fibronectin, the spaces collapse, and the tissue stiffens.
Vitamin D is squarely antifibrotic in this pathway. In nasal polyp-derived fibroblasts, 1,25(OH)₂D₃ suppresses α-SMA expression, fibronectin, total collagen production, collagen contraction, and cell migration in TGF-β1-induced cultures, acting through Smad2/3.
The same logic applies to the lung, where idiopathic pulmonary fibrosis is itself classified as a fibrosing interstitial pneumonia, and VDR agonists like paricalcitol suppress ER stress and JAK1/STAT3 activation in lung fibroblasts and reduce bleomycin-induced collagen deposition in the interstitium. Parallel work exists in liver, kidney, and cardiac fibrosis. So under the new framing, "vitamin D suppresses fibrosis" is also "vitamin D protects the integrity of the interstitial fluid compartment."
The second connection, and the one I think you'll find more interesting, is the free vitamin D hypothesis mapped onto interstitial space. The 25(OH)D in serum is ~85–90% DBP-bound, ~10–15% albumin-bound, and well under 1% free.
Only the free fraction crosses into tissue, equilibrates in interstitial fluid, and reaches the cells that actually express VDR — and several papers show the bioavailable and free concentrations correlate to clinical outcomes better than total 25(OH)D, though they remain hard to interpret because their values are three to four orders of magnitude lower than total concentrations and reference ranges are not established.
If you take the Benias/Theise reframing seriously, the interstitium is the spatial compartment where free vitamin D does its work. That makes the
- megalin/cubilin shuttle,
- extrarenal CYP27B1 activation in macrophages, and
- intracrine/paracrine signaling
all interstitial phenomena. The pharmacokinetics didn't change, but the anatomical picture is now a continuous, body-wide fluid network rather than a vague "tissue space" — which is actually a more honest model of where dissolved 25(OH)D and locally produced 1,25(OH)₂D₃ live and act.
The third, more speculative connection is immune trafficking and the lymphatic continuum. Dendritic cells, macrophages, and T cells migrate through interstitial channels to draining lymph nodes; vitamin D modulates DC maturation, T-reg induction, and macrophage polarization. Locally produced 1,25(OH)₂D₃ from macrophage CYP27B1 would diffuse in interstitial fluid before being either degraded by CYP24A1 or acting on neighboring cells.
None of this is new vitamin D biology, but the interstitium framing gives it a cleaner spatial substrate. The cancer-metastasis angle from the original Benias paper could also tie in here, since vitamin D's effects on tumor cell invasiveness and on the pre-metastatic niche would be playing out in exactly the channels they identified.
What's missing — and this is where I'd flag the research gap — is any direct work asking whether the CD34+ fibroblast-like cells lining the interstitial spaces express VDR at distinctive levels, whether interstitial fluid 25(OH)D concentrations track serum free 25(OH)D as expected, or whether vitamin D status affects interstitial hydraulic properties (compliance, drainage rate, collagen crosslinking density). Those are answerable questions; nobody seems to have asked them in this framing. The "Bolus is Bogus" thread might actually intersect here too — if peak-and-trough dosing produces large swings in free 25(OH)D, the interstitial compartment is where those swings would equilibrate, and the kinetics of equilibration across a body-wide fluid network is not the same as the kinetics in serum.
Liters of fluids
Interstitial fluid ~10 liters. Makes up roughly 15% of body weight
Blood: ~5 liters. This is whole blood (plasma + cells). The plasma portion is ~3 liters and the cells ~2 liters. Blood volume scales with body size, roughly 7–8% of body weight.
Lymph: ~1–2 liters present in the system at any given moment. This one is fuzzier because lymph is constantly being formed and drained rather than sitting in a fixed reservoir. The more commonly cited figure is the flow: roughly 2–4 liters of lymph drain back into the bloodstream per day via the thoracic duct and right lymphatic duct.
To tie the compartments together, since you're building a picture of fluid distribution: the ~5 L of plasma water, ~10 L of interstitial fluid, and the lymph all interconnect. Plasma filters out of capillaries into the interstitial space, and the lymphatic system collects the excess interstitial fluid and returns it to the blood — closing the loop. The lymph "volume" is really just interstitial fluid in transit, which is why it doesn't have a crisp fixed number the way blood does.
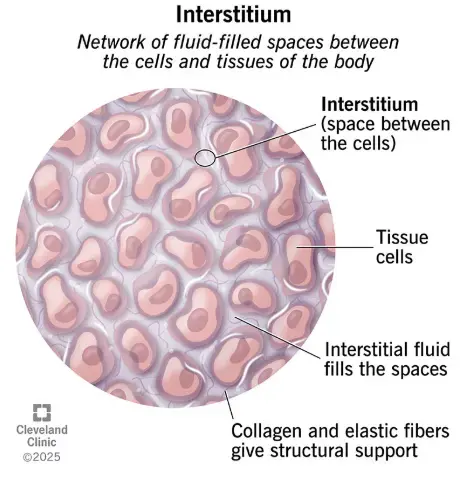
Definition and image
The interstitium is a contiguous, body-wide network of fluid-filled spaces supported by a mesh of strong collagen and elastin fibers. It surrounds blood vessels, lines the digestive tract, and sits just below the surface of our skin. Often described as an expansive, fluid-filled highway, it functions as a crucial shock absorber and acts as the primary source of lymph fluid