Bronchiolitis hospital stay cut by 2 days with 200,000 IU vitamin D – if deficient – RCT
Efficacy of vitamin D supplementation for children with acute bronchiolitis: A randomized controlled trial
World J Clin Pediatr. 2026 Mar 9;15(1):114465. doi: 10.5409/wjcp.v15.i1.114465.
Background: Previous studies have suggested an association between vitamin D deficiency and bronchiolitis, but the therapeutic benefits of vitamin D supplementation remain uncertain.
Aim: To investigate the efficacy of vitamin D supplementation for hospitalized children with acute bronchiolitis.
Methods: This two-arm randomized controlled trial included 146 children aged 3-24 months who were hospitalized with bronchiolitis at an Egyptian tertiary care center. Participants were equally randomized to receive a single intramuscular dose of 200000 IU (study group) or a daily oral dose of 400 IU (comparison group) of vitamin D3. The primary outcome was the time to hospital discharge. Secondary outcomes included time to oxygen weaning, discontinuation of intravenous fluids, and discharge readiness as well as serum 25-hydroxyvitamin D [25(OH)D] levels on day 3 post-randomization. Both the study and comparison groups were compared in the whole cohort (primary analysis) and within the subgroup of participants with baseline serum 25(OH)D levels < 30 ng/mL (prespecified subgroup analysis).
Results: In the overall analysis, the study and comparison groups showed no significant differences in median time to discharge (130 hours vs 140 hours, P = 0.149) or in secondary outcomes, except for a higher serum 25(OH)D level in the study group (51 ± 12.8 vs 32 ± 13.2 ng/mL, P < 0.001).
However, among the subgroup of participants with baseline serum 25(OH)D levels < 30 ng/mL, the study group demonstrated significantly:
1. shorter median times to hospital discharge (120 hours vs 170 hours, P < 0.001)
2. oxygen weaning (56 hours vs 79 hours, P = 0.012)
3. discontinuation of intravenous fluids (55 hours vs 73 hours, P = 0.017), and
4. discharge readiness (118 hours vs 165 hours, P = 0.001)
as well as a greater increase in serum 25(OH)D levels (40 ± 6.6 ng/mL vs 20 ± 6.1 ng/mL, P < 0.001) than the comparison group.
Conclusion: Vitamin D supplementation may improve clinical outcomes in hospitalized children with bronchiolitis who have vitamin D deficiency or insufficiency, supporting a test-and-treat approach.
Bronchiolitis etc. all prevented and/or treated by Vitamin D
Bronchiolitis — inflammation of the small airways (bronchioles), almost always viral (RSV most common), affects children under 2, causes wheezing and crackles, no specific treatment beyond supportive care.
Bronchitis — inflammation of the larger airways (bronchi), can be viral or bacterial, affects older children too, produces a productive cough but typically without wheezing. Bronchiolitis is often confused with this but is a distinct and more serious condition in infants.
Croup — viral inflammation of the upper airway (larynx and trachea), produces the characteristic "barking seal" cough and stridor (high-pitched inhaled sound), affects ages 6 months–3 years, responds to steroids and nebulized epinephrine.
Asthma — chronic inflammatory condition of the bronchi triggered by allergens, exercise, or infections, causes recurrent wheezing episodes, responds to bronchodilators and steroids. Distinguishing early asthma from recurrent bronchiolitis is a genuine clinical challenge.
Pneumonia — infection of the lung tissue (alveoli) itself rather than airways, bacterial or viral, causes fever, crackles, and consolidation on imaging, antibiotics work for bacterial cases.
RSV lower respiratory infection — RSV is the dominant cause of bronchiolitis but can also cause pneumonia in the same age group, sometimes used interchangeably with bronchiolitis in infants.
The key distinguishing features across all of these are the anatomical location (upper vs. lower airway, large vs. small airways, airways vs. alveoli), age of peak incidence, causative agents, and response to treatment.
Related in Vitamin D Life
- Topical Vitamin D provides more benefits than oral sometimes - many studies
- Topical vitamin D might be more bio-available than oral
- Topical vitamin D raised blood level to 38 ng (used Aloe Vera gel) – RCT
Response to injection is weeks
- Vitamin D supplementation protocols: loading, injection, etc – RCT
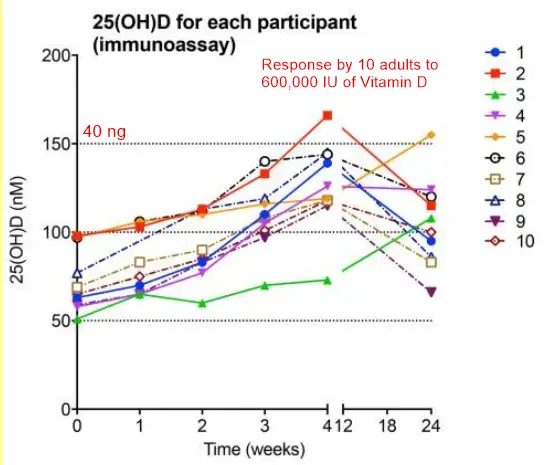
- Vitamin D injection of 600,000 IU (response by 10 individuals)
Response to injection takes about a month for those with strokes
- Megadose injection of up to 600,000 IU vitamin D3 every three months for adolescents - April 2010
- Preemies getting a 10,000 IU injection of vitamin D had far fewer breathing problems – RCT 2024
- TBI reduced 5X by 300,000 IU of vitamin D (injection) – RCT
- Injection
Bronchiolitis and RSV
- RSV kills 100,000 children annually around the world (Vitamin D can help)
- Tripledemic: Flu, COVID, and RSV (all fought by Vitamin D)
- Respiratory viral infection (RSV) and low vitamin D - many studies
- Vitamin D can inhibit enveloped virus (e.g. Corona, Herpes, Bird Flu, Epstein, Hepatitis, RSV, etc.)
- Bronchiolitis had 1.3 X longer hospitalization if low Vitamin D (1016 infants)
- RSV (bronchitis and viral pneumonia) in infants associated with low vitamin D and antibiotics
Response to Topical Vitamin D is hours, not weeks - far faster than injection
Topical Vitamin D: Nanoemulsion, Aloe Vera cream, patches, etc., probably provide a much faster response than injection.
- Topical vitamin D raised blood level to 38 ng (used Aloe Vera gel) – RCT
- Vitamin D3 Patch - expensive, many available
- Topical Vitamin D (nanoemulsion cream etc)
- Nanoemulsion Vitamin D is faster and better - many studies
- Inhaled nanoemulsion of Vitamin D killed lung bacteria
infants may not be able to inhale it however