60,000 IU of Vitamin D daily for 7 years treats many autoimmune diseases without toxicity (cofactors were used)
60,000 IU of Vitamin D Daily: 7 Years of Clinical Data Reveals the Truth
Why is 60,000 IU of vitamin D necessary for autoimmune disease patients
- The hypercalcemia myth: Real patient data showing D3 over 200 ng/mL with NORMAL calcium
- The 1928 Steck Report: 9-year study proving safety at 20,000 IU/kg body weight (completely buried)
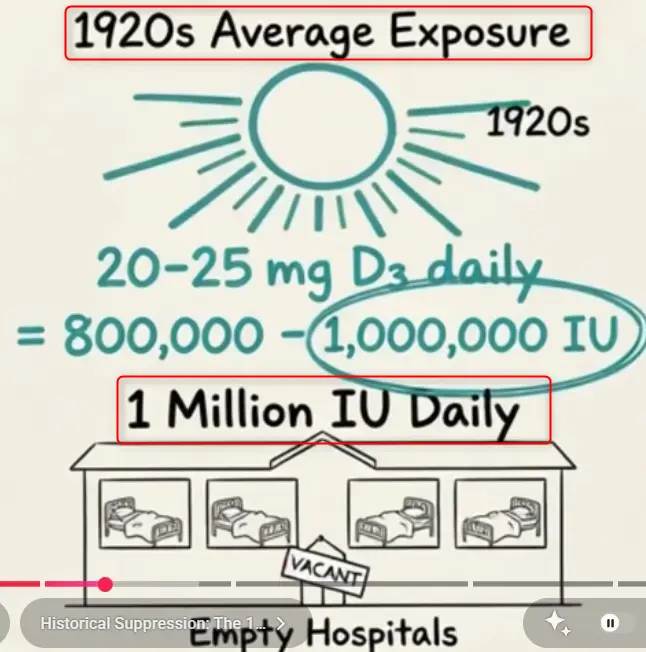
- Why were hospitals empty in the 1920s when people got 800,000-1,000,000 IU daily
- Our safety monitoring protocol: Ionized calcium, PTH, and kidney function
- Required cofactors: Why magnesium, K2, and others are non-negotiable
Real patient outcomes: MS remission, RA reversal, psoriasis clearance
His Indian Website on: Vitamin D, Autoimmune - many videos
Video summary by Claude AI May 2026
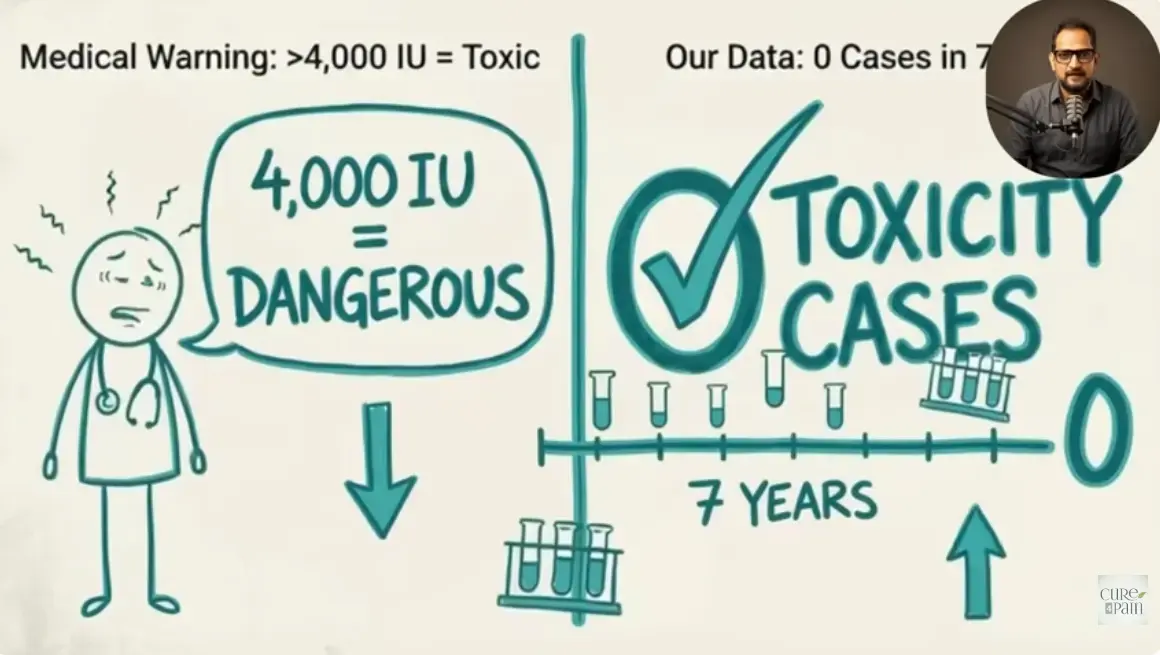
- [00:00–00:42] Clinical practice claim: After 7+ years of giving patients 60,000 IU vitamin D daily (sometimes for years), monitoring thousands with blood work every 3–6 months, the presenter reports zero cases of toxicity — challenging the standard 4,000 IU/day upper limit warning.
- [01:03–01:34] Target population: Patients with autoimmune diseases (MS, RA, psoriasis, lupus) typically prescribed lifetime biologics ($2,000–$5,000/month). Many reportedly achieve complete remission on the protocol.
- [01:34–02:43] Sample patient data: Vitamin D levels of 156–220 ng/mL with ionized calcium remaining in normal or low-normal range. Attributed to required cofactors — magnesium, vitamin K2, and boron — which direct calcium to bones rather than soft tissues. Hypercalcemia risk is framed as a result of isolated vitamin D dosing without cofactors.
- [02:49–03:53] Historical reference: Cites a 1928 "Dr. Steck" 9-year study (773 humans, 63 dogs) at 20,000 IU/kg, and claims 1920s populations got 800,000–1M IU daily from sun/diet with "empty hospitals" until 400 IU upper limits were introduced.
- [03:59–04:43] Rationale for high doses — "vitamin D resistance" in autoimmune patients caused by:
- (1) chronic infections creating gut biofilms that block absorption, - new to Vitamin D Life
- (2) VDR genetic polymorphisms,
- (3) metabolic syndrome damaging cellular machinery.
Vitamin D is framed as a steroid hormone regulating 2,700 genes.
- [04:43–05:50] Example RA patient workup showing low vitamin D (18 ng/mL), elevated PTH (89 pg/mL — interpreted as D3 resistance signal), elevated eosinophils, insulin resistance, and high triglycerides — justifying 60,000 IU three times per week.
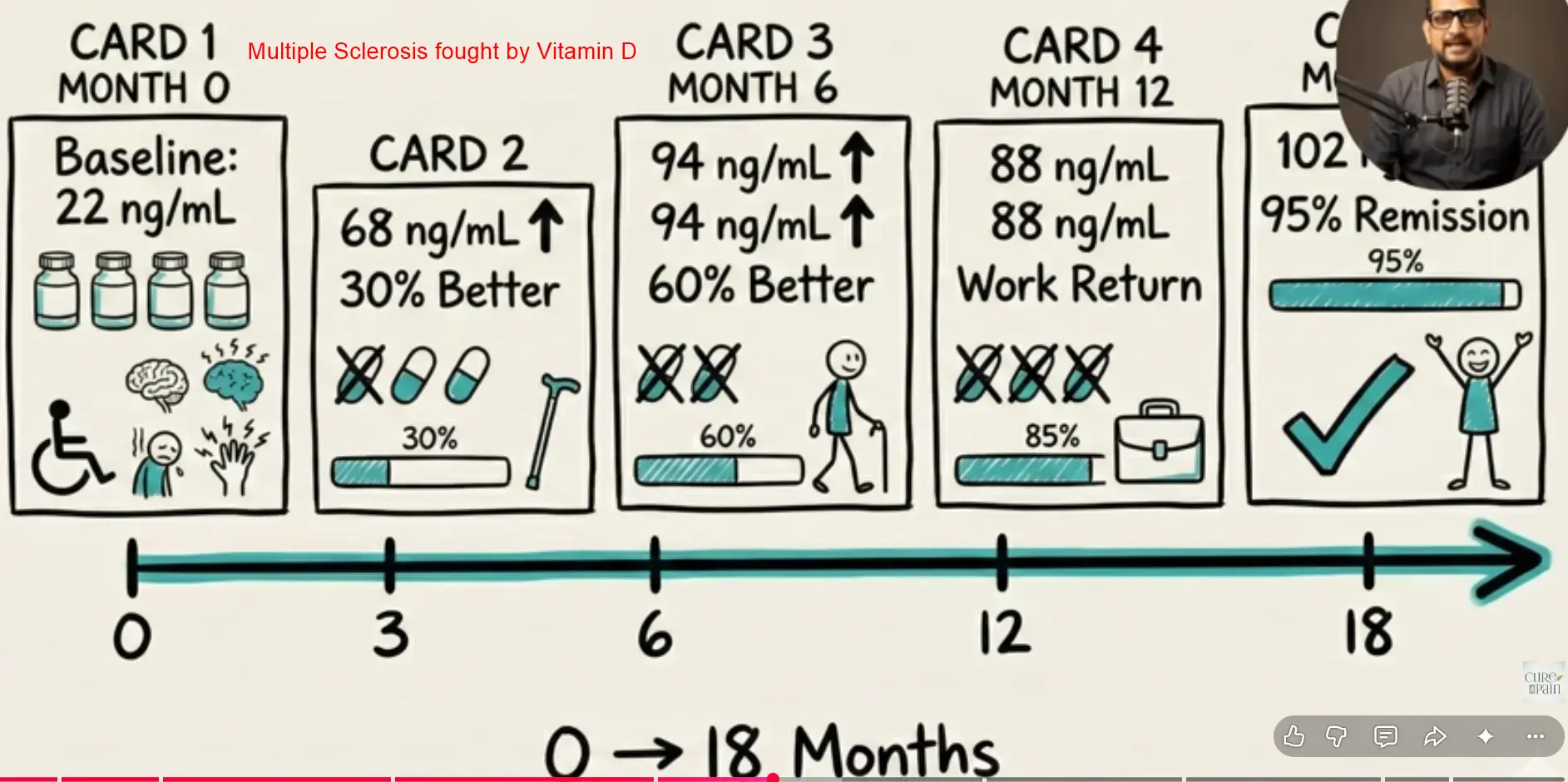
- [05:50–06:46] Illustrative MS case timeline: baseline vitamin D 22 ng/mL on 4 medications → month 18: 102 ng/mL, 95% symptom-free, off all pharmaceuticals.
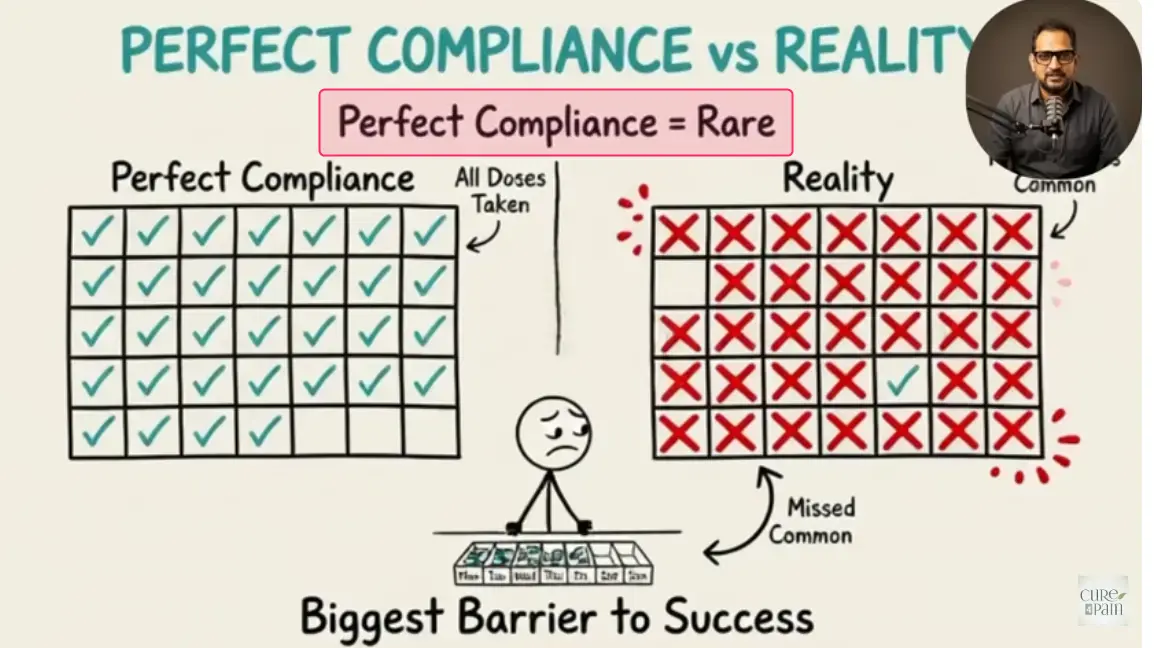
- [06:46–07:42] Biggest obstacle reported is patient compliance — daily supplements, quarterly bloodwork, and continuing through delayed symptom relief. Cognitive impairment from infections, premature discontinuation, and cost are common compliance failures.
- [07:44–08:33] Required monitoring every 3 months in year one: ionized calcium (not total), PTH (the "safety canary"), kidney function (creatinine, GFR), vitamin D, CBC, and inflammatory markers. Safety threshold defined as normal PTH + non-elevated ionized calcium.
- [08:33–09:20] Mandatory cofactors: magnesium glycinate 400–800 mg/day, vitamin K2 MK-7 ~100 mcg/day, B-complex, mineral balance, omega-3s, and absorption enhancers (TUDCA, betaine HCl). Framed as "ecosystem restoration," not vitamin D monotherapy.
- [09:20–10:16] Cost comparison: ~$55–110/month supplements plus ~$60 quarterly labs (pricing given in rupees, suggesting India-based practice), versus $2,000–$5,000/month biologics.
Related in Vitamin D Life
- Cofactors are needed when taking high-dose vitamin D - video
- Coimbra high-dose vitamin D protocol - many studies
He also recommends increasing cofactors, increasing water, and decreasing Calcium - The BEST Nutrient for Autoimmune Conditions (Vitamin D) - video
- Coimbra protocol using high-dose Vitamin D is safe
- Note: India uses 60,000 IU packets; most of the world uses 50,000 IU
- 50,000 IU and other high dose vitamin studies
- Comparing High-dose vitamin D therapies
All of the therapies use cofactors, some of which keep Calcium away from soft tissues - Vitamin D Toxicity is rare – only 1 unknown case in 74,000 patients
Cofactors
- Less Calcification if less Calcium or more Vitamin K, Magnesium, etc. - many studies
- Vitamin D Cofactors in a nutshell
Vitamin D Resistance