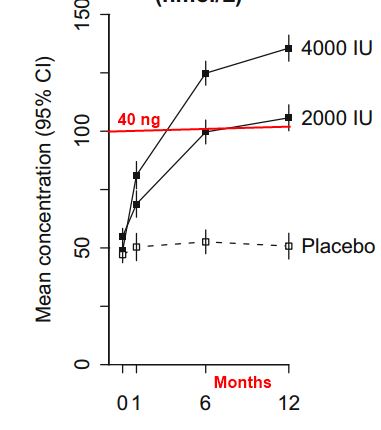
4,000 IU of Vitamin D daily is safe, but takes a year to plateau (Best-D) – RCT
Optimum dose of vitamin D for disease prevention in older people: BEST-D trial of vitamin D in primary care
Response was still increasing at 12 months
See also Vitamin D Life
Note: this study was looking at Vitamin D safety for Osteoporosis
Osteoporosis helped by Vitamin D, still not willing to recommend exact dose size – Nov 2016
Osteoporosis treatment guidelines by US Endocrinology groups – Sept 2016
Even taking as much as 4200 IU vitamin D 43 percent had less than 30 ng in blood – RCT Jan 2013
Overview Loading of vitamin D Get Vitamin D benefit in 5-20 days instread of 100-300 days
Seniors need at least 4,000 IU vitamin D, no test needed – Consensus Jan 2014
4,000 IU of Vitamin D - many pages
Overview Osteoporosis and vitamin D contains the following summary
{include}
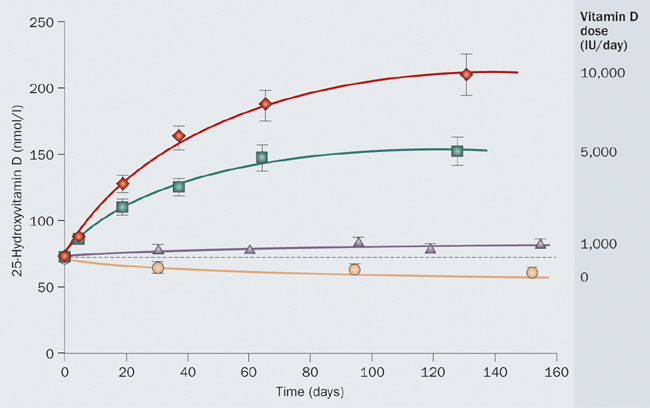
Overview Vitamin D Dose-Response has the following chart
_
Note the increase between triangles at 6 months and circles at 12 months

In 3 studies people have taken 12 months to plateau
However, typically studies show the response leveling out at about 3 months
Osteoporosis International pp 1–11, First Online: 16 Dec 2016, DOI: 10.1007/s00198-016-3833-y
H. HinJ. TomsonC. NewmanR. KurienM. LayJ. CoxJ. SayerM. HillJ. EmbersonJ. ArmitageR. Clarke
📄 Download the BEST-D PDF from Vitamin D Life
Summary
This trial compared the effects of daily treatment with vitamin D or placebo for 1 year on blood tests of vitamin D status. The results demonstrated that daily 4000 IU vitamin D3 is required to achieve blood levels associated with lowest disease risks , and this dose should be tested in future trials for fracture prevention.
Introduction
The aim of this trial was to assess the effects of daily supplementation with vitamin D3 4000 IU (100 μg), 2000 IU (50 μg) or placebo for 1 year on biochemical markers of vitamin D status in preparation for a large trial for prevention of fractures and other outcomes.
Methods
This is a randomized placebo-controlled trial in 305 community-dwelling people aged 65 years or older in Oxfordshire, UK. Outcomes included biochemical markers of vitamin D status (plasma 25-hydroxy-vitamin D [25[OH]D], parathyroid hormone [PTH], calcium and alkaline phosphatase), cardiovascular risk factors and tests of physical function.
Results
Mean (SD) plasma 25(OH)D levels were 50 (18) nmol/L at baseline and increased to 137 (39), 102 (25) and 53 (16) nmol/L after 12 months in those allocated 4000 IU, 2000 IU or placebo, respectively (with 88%, 70% and 1% of these groups achieving the pre-specified level of >90 nmol/L). Neither dose of vitamin D3 was associated with significant deviation outside the normal range of PTH or albumin-corrected calcium. The additional effect on 25(OH)D levels of 4000 versus 2000 IU was similar in all subgroups except for body mass index, for which the further increase was smaller in overweight and obese participants compared with normal-weight participants. Supplementation with vitamin D had no significant effects on cardiovascular risk factors or on measures of physical function.
Conclusions
After accounting for average 70% compliance in long-term trials, doses of 4000 IU vitamin D3 daily may be required to achieve plasma 25(OH)D levels associated with lowest disease risk in observational studies.