Vitamin B12 as a Treatment for Pain – review
Pain Physician . 2019 Jan;22(1):E45-E52.
Buesing S1, Costa M1, Schilling JM1, Moeller-Bertram T1.

 1. Vitamin D, Vitamin B12, etc. charts- 2004-2018 has the following
1. Vitamin D, Vitamin B12, etc. charts- 2004-2018 has the following ---* Dr. Coimbra discusses Vitamin D, Magnesium, Folic Acid, B12, Autism, Depression, etc – Sept 2018* Autism treated by Vitamin B12 - several studies* Sleep, Vitamin D, Vitamin B-12, IBS, Fibromyalgia - Gominak March 2015* Hypothesis – Vitamin B-12 deficiency is associated with Vitamin D deficiency Gominak
---* Dr. Coimbra discusses Vitamin D, Magnesium, Folic Acid, B12, Autism, Depression, etc – Sept 2018* Autism treated by Vitamin B12 - several studies* Sleep, Vitamin D, Vitamin B-12, IBS, Fibromyalgia - Gominak March 2015* Hypothesis – Vitamin B-12 deficiency is associated with Vitamin D deficiency Gominak📄 Download the PDF from Vitamin D Life
BACKGROUND: First isolated as cyanocobalamin in 1948, vitamin B12 has been explored for pain treatment almost since its discovery. With the advent of the opioid epidemic, safer treatments for pain are needed.
OBJECTIVES: Our objective was to compile the latest information on potential mechanisms from animal studies and clinical trial data on vitamin B12 for the treatment of pain conditions.
STUDY DESIGN: We conducted a narrative review.
METHODS: PubMed was searched using the terms
"methylcobalamin pain",
"hydroxycobalamin pain",
"cyanocobalamin pain", and "vitamin B12 pain."
Animal studies that identified mechanisms of action for the effects of pain were collected. Clinical trials utilizing larger, pharmaceutical doses of vitamin B12 (> 100 µg/dose) in pain treatment were identified and reviewed.
RESULTS:
Animal studies support multiple beneficial effects of vitamin B12 including the regeneration of nerves and the inhibition of cyclooxygenase enzymes and other pain-signaling pathways. In addition, animal studies have demonstrated synergistic benefits of vitamin B12 combined with other pain medications, including nonsteroidal anti-inflammatory drugs and opiates. Clinical trials provide evidence for the effectiveness of vitamin B12 for the treatment of low back pain and neuralgia, although data is still fairly limited and optimal treatment regimens have not been identified.
LIMITATIONS: More large, double-blind placebo-controlled trials are needed to fully establish efficacy and best dosing parameters.
CONCLUSION:
Vitamin B12 may prove to be an adjunctive or integrative treatment for pain conditions. While more research is needed, considering the low incidence of side effects and overall safety, B12 may be an additional tool to consider for pain treatment.
Text extracted from PDF
Vitamin B12 was initially discovered more than 70 years ago during a search for the "anti- pernicious anemia factor" found in liver extracts used to treat pernicious anemia (1,2). Since that time, it has become apparent that vitamin B12 has numerous physiological effects, many of which support nervous system functioning. In the 1950s, researchers
began to focus on pain-relieving effects from vitamin B12 administration with some potentially impressive clinical results (3,4), although study methodologies were not robust and some studies on other pain conditions showed no effects (5). Unfortunately, over the ensuing decades interest in clinical uses of vitamins and minerals waned in favor of pharmaceutical treatments. Now, with the advent of the opioid epidemic, alternative and complementary approaches to pain relief are needed more than ever to help reduce the use of and reliance on opioid medications. In the current published literature, vitamin B12 has been used as a treatment for patients with chronic pain conditions including diabetic neuropathy (6-8), postherpetic neuralgia (9), low back pain (10,11) and aphthous ulcers (12), all with significant results.
Methods
Initially, for inclusion in this review, PubMed was searched using the terms "methylcobalamin pain", "hydroxycobalamin pain", "cyanocobalamin pain", and "vitamin B12 pain." Primary animal studies exploring the mechanisms of effect of B12 on pain and clinical studies using higher pharmacological dosing of vitamin B12 (> 100 pg/dose) for pain were identified, included, and reviewed. In addition, a review of the basic history and biochemistry of B12 was also included from available resources.
Results
Vitamin B12 Biochemistry
Vitamin B12 is the largest and most complex vitamin in the human body. Its structure consists of a corrin ring similar to hemoglobin and chlorophyll. In vitamin B12, the active site utilizes cobalt, which binds different chemical groups including cyano, hydroxy, methyl, and 5'-deoxyadenosyl, the latter 2 being the active vitamin B12 moieties utilized in the human body to catalyze specific enzymatic reactions.
Vitamin B12 is normally acquired through food. It is typically bound to protein and requires stomach acid and the digestive enzyme pepsin to release it in free form. Vitamin B12 then combines with intrinsic factor produced from the stomach and is absorbed in the small intestine. A small percentage of free form vitamin B12 can diffuse directly through the intestinal barrier as well (13). Medications and some medical conditions can decrease absorbance and increase the risk of vitamin B12 deficiency. Stomach acid-lowering medication, including proton pump inhibitors (14) and histamine H2-receptor antagonists (15), can both lead to deficits in B12 absorption and deficiency. Weight loss surgery (16) also decreases the absorption of vitamin B12, as do other gastrointestinal conditions including inflammatory bowel disease (17).
In humans, vitamin B12 catalyzes methyl transfers and isomerase reactions. Isomerase reactions that involve the enzyme methylmalonyl-CoA mutase (also called methylmalonyl-CoA isomerase) utilize vitamin B12 as adenosylcobalamin and are required for the metabolism of odd chain fatty acids, isoleucine, methionine, threonine, valine, and cholesterol (18).
Methionine synthase, a methyltransferase, is the main enzyme in humans that utilizes methylcobalamin as a methyl source and provides for methylation reactions throughout the body. The amino acid methionine is produced from homocysteine by adding the methyl group from the active form of vitamin B12 methylcobalamin. Folic acid, in the form of methyltetrahydrofolate, is then required to recycle vitamin B12 back to its active methylated form, as shown in Fig. 1. Methionine from this reaction is then converted to S-adenosyl methionine (SAMe), one of the major methyl donors for methylation reactions throughout the body, including the methylation of myelin basic protein (19) and DNA (20). Myelin basic protein makes up a significant percentage of the myelin sheath around nerves and requires methylation for its stability. Nerve damage related to vitamin B12 deficiency appears to be a direct result of the body being unable to keep myelin basic protein methylated, leading to degeneration of the myelin sheath (19).
Effects and Mechanisms of Vitamin B12 on Pain
Vitamin B12 has a proclivity for neural tissue. Initial animal models suggest that B12 helps to regenerate nerves by inducing axonal growth and Schwann cell differentiation, which improves functional recovery in difficult-to-treat nerve crush injuries (21-23). In addition, B12 upregulates brain-derived neurotrophic factor (BDNF) and increases nerve conduction velocity, which may reflect part of the regeneration process (24,25).
Another potential mechanism of action for the pain-reducing properties of vitamin B12 comes from interactions with prostaglandin synthesis, including cyclooxygenase (COX) enzymes. Animal studies exploring the direct effects of vitamin B12 on COX enzyme are lacking. However, in rats, dextran sodium sulfate- induced colitis showed that a methyl-deficient diet (excluding vitamin B12, folate, and choline) caused a significant upregulation of COX2 in the intestines after dextran sodium sulfate exposure. It is possible that vitamin B12 may be one factor that helps keep COX2 levels in check during inflammatory challenges (26).
Additionally, several other lines of evidence suggest mechanisms involving COX enzymes and vitamin
B12. Orofacial pain induced by injecting formalin into the upper lip of rats causes 2 distinct phases of pain, the second phase mediated by COX enzymes. Nonsteroidal anti-inflammatory drugs (NSAIDs), which work through inhibiting COX enzymes, primarily reduce the second phase of orofacial pain after injections of formalin (27). Interestingly, vitamin B12 also powerfully reduces the second phase of formalin-induced orofacial pain, suggesting a similar interaction with COX enzyme systems (28). In hot-plate and abdominal writhing pain studies, mice showed mild and moderate pain reduction, respectively, in response to B12. Hot-plate pain testing involves central COX mechanisms, whereas abdominal writhing measures peripheral COX enzyme effects, indicating that B12 may have both central and peripheral COX inhibiting properties (29).
An additional potential pain relief mechanism involving neurotransmitters in humans has been proposed for vitamin B12. Studies using vitamin B1, B6, and B12 in combination are hypothesized to increase the production of or potentiate the pain inhibitory response of noradrenaline and 5-hydroxytryptamine (30). Evidence indicates that homocysteine decreases neurotransmitter synthesis (31,32), and it is well-documented that B vitamins decrease homocysteine (33). Lowering homocysteine with B vitamins might restore neurotransmitter production in individuals with elevated homocysteine, which could contribute to neurotransmitter-moderated pain reduction.
There are also data showing that vitamin B12 may function through interactions with the capsaicin receptor (TRPV1). TRPV1 is a receptor involved in pain processing, responding to heat, acid, and capsaicin - the compound that gives hot peppers their kick - with an influx of positive ions into the cell, which produces a sensation of burning pain. Vitamin B12 appears to reduce TRPV1 effects, decreasing pain signaling. In a mouse model, heat hyperalgesia was reduced with vitamin B12 through what appeared to be a reduction in TRPV1 influx (34).
Finally, vitamin B12 appears to have synergistic effects when combined with opiates for pain (29,35-37). In mice, administration of vitamin B12 and morphine resulted in a significant reduction of tolerance to morphine. In addition, B12 was shown to reduce morphine dependence (35). Combined B vitamins show similarly significant benefits of Vitamin B1, B6, and B12 administered with morphine, decreasing pain more than morphine alone. One study showed decreased tolerance to morphine with this B-vitamin combination as well (36,37).
Human Trials and Vitamin B12
There are studies showing pain benefits in humans with vitamin B12 administration. Admittedly, study methodology in some of the human trials has not been robust. However, considering the safety profile and the combination of animal and human studies in total, beneficial effects in select patient populations appear plausible with minimal risks.
B12 in Neuropathy/Neuralgia
Nerve crush injuries can cause significant damage that leads to lifelong morbidity. In a recent doubleblind, randomized, comparative study, 2 mg of oral hydroxycobalamin 3 times per day was compared to 2 mg of hydroxycobalamin with supplemental nucleotides (5 mg of CMP and 3 mg of UTP) 3 times per day in patients with compressive neuralgias. While there was no placebo group, high doses of hydroxycobalamin alone led to a 30.5-point (60%) drop in pain scores as assessed on a visual analog scale and a 35.2-point (69%) decrease when combined with the supplemented nucleotides (38).
Another comparison trial exploring vitamin B12 alone compared to vitamin B12 with acupuncture for chemotherapy-induced peripheral neuralgia in multiple myeloma showed benefits in pain reduction as well. Patients were given 500 pg methylcobalamin injections every other day for a total of 10 injections followed by oral methylcobalamin 500 pg 3 times per day for 2 months with or without acupuncture treatment. In patients receiving the methylcobalamin alone, pain scores had decreased significantly by 23% at the end of treatment (39).
In diabetic neuropathy there are a number of human trials showing positive outcomes. In a double-blind placebo-controlled trial, oral methylcobalamin at 1500 pg daily after 3 months yielded significant improvements in 2-point discrimination, muscle cramps and pain, with pain being reduced by 70%. Additionally, there was significant improvement in the conduction velocity and scalp somatosensory response of the median nerve, although these parameters did not change significantly in the lateral popliteal or posterior tibial nerves (6). In a similar double-blind, placebo-controlled trial, dosing 500 pg 3 times daily after 4 months showed significant reductions in somatic symptoms, autonomic symptoms, and a regression in the signs of diabetic neuropathy. The main study drawback was that it did not include a comparison to the placebo group (7). In a nonblinded trial using oral methylcobalamin 500 pg 3 times a day as an active comparison to intravenous prostaglandin treatment for diabetic neuropathy, oral methylcobalamin after 4 weeks showed 50% improvement in somatosensory symptoms but no benefit for vibratory threshold (8). In another comparison trial, vitamin B12 compared to alpha lipoic acid for diabetic neuropathy showed statistically significant pain improvement (40). In addition, combination trials in which vitamin B12 was used in significant doses in conjunction with other treatments (most often other B vitamins, including vitamin B1 and vitamin B6) also showed benefits for diabetic neuropathy (41-43).
Data exists supporting methylcobalamin as a treatment for herpetic neuralgia. In a randomized controlled trial, patients with herpetic neuralgia received either injections of 500 pg of methylcobalamin or lidocaine subcutaneously in 4 separate locations on the affected dermatome or oral methylcobalamin 500 pg 3 times a day. While lidocaine and oral methylcobalamin had small but significant effects on pain, daily injections of B12 reduced pain by half or more in 60% of subjects (9). In additional studies by the same author, B12 injections combined with lidocaine or vitamin B1 were used for herpetic itching and neuralgia, both studies showing clinically significant benefits (44,45).
Older studies reporting clinical experiences rather than controlled trials describe good efficacy with B12 injections for treating Morton's neuralgia and tabes dorsalis. A protocol for injecting B12 weekly into the third and fourth interspaces of patients with Morton's neuralgia was reported to resolve pain for 73% of 85 patients (4). Tabes dorsalis is a condition caused by nerve damage from tertiary syphilis that includes "lightning pains." Treatment of tabes dorsalis can be difficult, even with opioids, yet some patients were reported to receive highly significant pain reduction with injected B12 (3).
Low Back Pain
Low back pain is the second most common cause of disability in the US and costs $100-200 billion dollars per year in lost productivity, wages, and other costs (46). Low back pain is a large burden on society, which could benefit from additional safe and effective treatments.
In a randomized placebo-controlled double-blind study, injectable vitamin B12 as 1000 pg of cyanocobalamin (with a small amount of phospholipids) was given intramuscularly once daily for 2 weeks. Both active and placebo treatments yielded pain reductions; however, the active treatment performed significantly better, with pain scores decreasing by 87%. On the disability questionnaire, scores in the vitamin B12 group significantly decreased by 82%. From the data, cyanocobalamin, which is generally considered one of the more inferior treatment forms of vitamin B12, appeared to provide fairly rapid relief from chronic low back pain (10).
In a similar randomized, placebo-controlled trial for chronic back pain, 500 pg of intramuscular methylcobalamin was given 3 times per week for 2 weeks. While the placebo led to nonsignificant reductions in disability and pain, the active treatment reduced the disability score by 27% and the pain score by 31% (11).
In addition, studies using oral doses of B vitamins including B12 have shown synergistic effects with diclofenac for low back pain. In some studies, the combination improved functioning, while in others, the combination allowed for a reduction in the dose of diclofenac (47-49).
Aphthous stomatitis
Aphthous stomatitis (canker sores) are a fairly common painful oral pathology that can cause significant morbidity. While aphthous stomatitis is significantly different than the other pain conditions already discussed, it is worth noting that vitamin B12 still has significant pain-reducing effects. There are a number of studies documenting healing of aphthous ulcers using oral B12 as a topical treatment regardless of serum B12 levels. However, one recent study focused specifically on pain relief using topical B12 in combination with a topical steroid, compared to the topical steroid treatment alone. After 2 days of treatment, pain scores decreased significantly, dropping almost 94%, with some patients being completely pain-free in the B12 group.
In the control group, no one achieved full pain relief, with an average reduction of pain close to 65% (12).
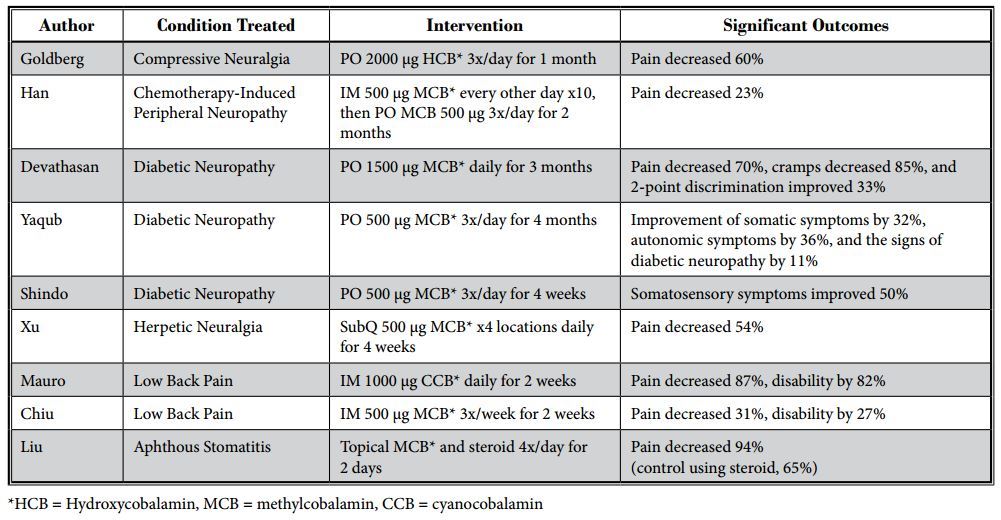
A summary of the clinical trials for treating pain conditions is listed in Table 1.
Discussion
Based on the available data, vitamin B12 as a treatment for chronic pain conditions may be an option for some patients. Animal models show multiple effects of vitamin B12 that are likely of clinical relevance, including the potential to support nerve regeneration, which could result in long-term healing beyond immediate pain-reducing effects.
Table 1. Summary of vitamin B12 clinical trials for pain conditions.
It is worth noting that vitamin B12 for pain is not limited in efficacy to treating patients with vitamin B12 deficiency. Doses of vitamin B12 in many of the clinical trials were typically above the threshold necessary to treat deficiency and most of the patients in the studies were not vitamin B12 deficient. The effects of vitamin B12 seem to occur through the vitamin's proclivity to support the nervous system and its anti-inflammatory effects. In addition, animal studies suggest that vitamin B12 may provide an opioid sparing effect, allowing for the reduction of opioid dose when used in combination for pain conditions. However, no human clinical trials were found that combine opioids and vitamin B12. Human clinical trials could help establish the efficacy of any opioid sparing effects of vitamin B12 for patients with chronic pain.
Dosing
When treating with vitamin B12, there may be a threshold at which the pharmacological effects of B12 more fully manifest. The studies by Mauro and Chiu exploring vitamin B12 and chronic low back pain showed that daily injections of 1000 pg of cyanocobalamin yielded around 80% reduction in chronic low back pain, whereas injections 3 times per week of 500 pg of methylcobalamin yielded around 30% reduction of pain (10,11). While the suggested threshold is intriguing, the studies were not identical. Outcomes from the study of B12 injections 3 times per week were assessed 2 months after the final injection, whereas the study using daily injections only evaluated patients at the end of injection therapy with no long-term follow-up after treatment. Larger trials with differing treatment regimens are still needed to fully assess the best approach for the use of vitamin B12 for different chronic pain conditions.
Safety
While vitamin B12 orally or by injection is typically well-tolerated with a low incidence of adverse events (50), there are rare case reports of allergic reactions, anaphylaxis, and other side effects. In most reports of anaphylactic reactions to injected B12, high-dose oral supplementation is still tolerated. However, there are exceptions noted in the literature (51). Although, desensitization protocols for reversing IgE-mediated allergy to B12 have also shown success (52). Other rare, but potential side effects include a small but significant drop of potassium in patients with macrocytic anemia and low serum potassium, which in extreme cases could be fatal. In patients with severe macrocytic anemia with hematocrit under 25%, vitamin B12 injections were shown to drop potassium levels initially by an average of 0.4 mEq/L since potassium is utilized in the production of red blood cells (53). Potassium should be monitored in this subset of patients. There are case reports of acne-like, voluminous folliculitis after intramuscular B12 that clears readily upon discontinuation (54). Dry mouth, nausea, and blurred vision have also been reported with B12 (55). An additional study using vitamin B6, B12, and folic acid in diabetic nephropathy showed decreased kidney function and increased cardiovascular events with the vitamins, although the study only included 118 patients for the primary outcome at 36 months (56). A separate study of 2056 patients with nephropathy followed for over 3 years, including a subset with diabetic nephropathy, showed no significant impact of these same vitamins on mortality, cardiovascular, or other secondary outcomes (57). Drug references list congestive heart failure and pulmonary edema as serious adverse events, yet a review of the literature did not turn up any case reports.
Conclusion
While older reviews of vitamin B12 for pain exist, conclusions have varied. Most reviews showed positive results while recognizing lower study quality or the need for further research (58,59). One recent review concluded that there was no evidence of any benefits of oral supplementation of B12 in diabetic neuropathy (60). The review included 4 studies, one of which used a very low dose of B12 (20 pg) that is likely below the benefit threshold for vitamin B12. Interestingly, the other 3 studies (included in the above review) showed a statistically significant benefit of B12 treatment and all 3 concluded that B12 alone or in combination with other nutrients significantly improved multiple endpoints for diabetic neuropathy (7,42,43).
Looking at the sum total of research based on the mechanistic studies and human clinical trials, evidence suggests that vitamin B12 has at least modest pain- relieving properties. Additional placebo-controlled human trials with dose response regimens for different pain conditions would help to elucidate the conditions and treatment protocols that best utilize its effects.
The challenges of treating chronic pain have led us to the current opioid crisis with high costs in terms of dollars and lives lost. Additional, safe treatments for chronic pain like vitamin B12 need more research and potential utilization to provide additional and safe stand-alone or adjunctive treatment options for chronic pain.
Disclosures and Acknowledgments
The authors have nothing to disclose. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.