Supplements - why and which
Why US Adults Use Dietary Supplements
JAMA Intern Med. Published online February 4, 2013. doi:10.1001/jamainternmed.2013.2299 Regan L. Bailey, PhD, RD; Jaime J. Gahche, MPH; Paige E. Miller, PhD, RD; Paul R. Thomas, PhD, RD; Johanna T. Dwyer, PhD, RD
PDF is attached at the bottom of this page
Background: Dietary supplements are used by more than half of adults, although to our knowledge, the reasons motivating use have not been previously examined in US adults using nationally representative data. The purpose of this analysis was to examine motivations for dietary supplement use, characterize the types of products used for the most commonly reported motivations, and to examine the role of physicians and health care practitioners in guiding choices about dietary supplements.
Methods: Data from adults (>20 years; n = 11 956) were examined in the 2007-2010 National Health and Nutrition Examination Survey, a nationally representative, cross-sectional, population-based survey.
Results: The most commonly reported reasons for using supplements were to "improve" (45%) or "maintain" (33%) overall health. Women used calcium products for "bone health" (36%), whereas men were more likely to report supplement use for "heart health or to lower cholesterol" (18%). Older adults (>60 years) were more likely than younger individuals to report motivations related to site-specific reasons like heart, bone and joint, and eye health. Only 23% of products were used based on recommendations of a health care provider . Multivitamin-mineral products were the most frequently reported type of supplement taken, followed by calcium and w-3 or fish oil supplements. Supplement users are more likely to report very good or excellent health, have health insurance, use alcohol moderately, eschew cigarette smoking, and exercise more frequently than nonusers.
Conclusions: Supplement users reported motivations related to overall health more commonly than for supplementing nutrients from food intakes. Use of supplements was related to more favorable health and lifestyle choices. Less than a quarter of supplements used by adults were recommended by a physician or health care provider.
Author Affiliations: Office of Dietary Supplements (Drs Bailey, Thomas, and Dwyer) and National Cancer Institute (Dr Miller), National Institutes of Health, Bethesda, Maryland; National Center for Health Statistics, Centers for Disease Control and Prevention, Hyattsville, Maryland (Ms Gahche); and Jean Mayer USDA Human Nutrition Research Center on Aging at Tufts University and School of Medicine and Friedman School of Nutrition Science and Policy, Tufts University, Boston, Massachusetts (Dr Dwyer).
DIETARY SUPPLEMENT USE among adults has increased over the past 30 years in the United States,1,2 and currently about half of adults report using 1 or more dietary supplements.3,4 Many characteristics of people who choose supplements are known: users tend to be older,2,3,5 have a lower body mass index (BMI)5,6 (calculated as weight in kilograms divided by height in meters squared), are more physically active,5,7 are less likely to smoke,7,8 and have higher educational attainment and socioeconomic status compared with nonusers.6,9 However, the actual motivations for use, that is, the reasons that people take dietary supplements remain unclear. The National Health and Nutrition Examination Survey (NHANES) began querying motivations for use of dietary supplements for the first time in 2007. The purpose of this analysis was to examine motivations for use of dietary supplements by adults as well as to characterize the types of products that were used and the most common motivations for using them in the 2007-2010 NHANES.
METHODS
The NHANES is a nationally representative, cross-sectional survey that samples noninstitutionalized, civilian US residents using a complex, stratified, multistage probability cluster sampling design collected by the National Center for Health Statistics (NCHS).10 Data used for the present analysis were from the household interviews (n = 20 686; 10 149 from 2007 to 2008 and 10 537 from 2009 to 2010). Those younger than 20 years (n = 8533), lactating (n=63), and/or pregnant women (n= 125), and those with unknown or missing supplement information (n=9) were excluded. The final analytic sample was n=11 956. Written informed consent was obtained for all participants, and the survey protocol was approved by the research ethics review board at the NCHS.
Demographic data were collected through a computer-assisted personal interview. Three racial/ethnic groups are available in the 2007-2010 NHANES: non-Hispanic whites, non-Hispanic blacks, and Hispanics. The poverty income ratio (PIR) is a measure that represents the ratio of household income to the poverty threshold after adjustments for inflation and family size. Three PIR categories were constructed: less than 130%, 130% to 250%, and more than 250%. Measured height and weight were used to calculate BMI, and the following classifications were used: obese (>30.0), overweight (25.0-29.9), normal weight (18.5-24.9), and underweight (<18.5).
The Dietary Supplement Questionnaire (DSQ) was used to collect detailed information on the participant's use of vitamins, minerals, herbals, and other supplements over the past 30 days. Broad mutually exclusive supplement categories were constructed based on nutrient content and/or descriptive characteristics commonly used in marketing (eTable; http://www.jamainternalmed.com ). Motivations were also assessed using a categorical question that included reasons for use for each reported supplement using a hand card with a list of possible reasons. Participants were able to choose more than 1 reason. Participants were also able to provide their own reasons. Participants were also asked if they used the supplement for their own reasons or based on the advice of a health care provider.
Self-reported exercise patterns were obtained from the physical activity questionnaire. Activity was classified as low, moderate, or high intensity. Alcohol use in the past 12 months was dichotomized into yes or no; the average number of drinks reported per day was categorized as 0 (ie, those not reporting use in the past 12 months), 1, 2, or 3 or more drinks per day. Smoking was categorized as "never," "former," "current/ occasional," and "current/daily." Self-reported health was classified as excellent/very good, good, or fair/poor.11
STATISTICAL ANALYSIS
All statistical analyses were performed using SAS software (version 9.3; SAS Institute Inc) and SAS-callable SUDAAN software (version 10; Research Triangle Institute). Sample weights were used to account for differential nonresponse and noncov-erage, and to adjust for planned oversampling of some groups. Standard errors (SEs) for all statistics of interest were approximated by Taylor Series Linearization. Motivations for use of dietary supplements are presented only for users of supplements (n= 5514). Contrast statements in Proc Descript command were constructed to examine demographic and lifestyle differences related to supplement use; P < .05 was considered statistically significant.
From 2007 through 2010, 49% (SE, 1%) of adults reported using a dietary supplement product within the past 30 days; this was more common in women than men (Table 1). Older adults (> 60 years) and non-Hispanic whites reported higher use than the younger age groups and other races, respectively. Individuals classified as underweight or obese were less likely to use supplements than normal and overweight individuals. Supplement use was also significantly different across all PIR and smoking categories. Those with health insurance were much more likely to report supplement use than those without insurance. Supplement use was also lower in those with low reported exercise, higher in those who reported 1 alcoholic drink per day, and higher among those who reported excellent or very good health
(Table 1).
Table 1.
Prevalence of Dietary Supplement Use by Demographic, Anthropometric, Socioeconomic, and Lifestyle Characteristics Among Adults ( 20 Years) in the United States, 2007-20101,2
Abbreviations: BMI, body mass index (calculated as weight in kilograms divided by height in meters squared); SE, standard error.
a Data are presented as percentages (SE); sample size is 11 956 unless otherwise noted.
b Estimates with different letter subscripts are significantly different within a category; P< .05.
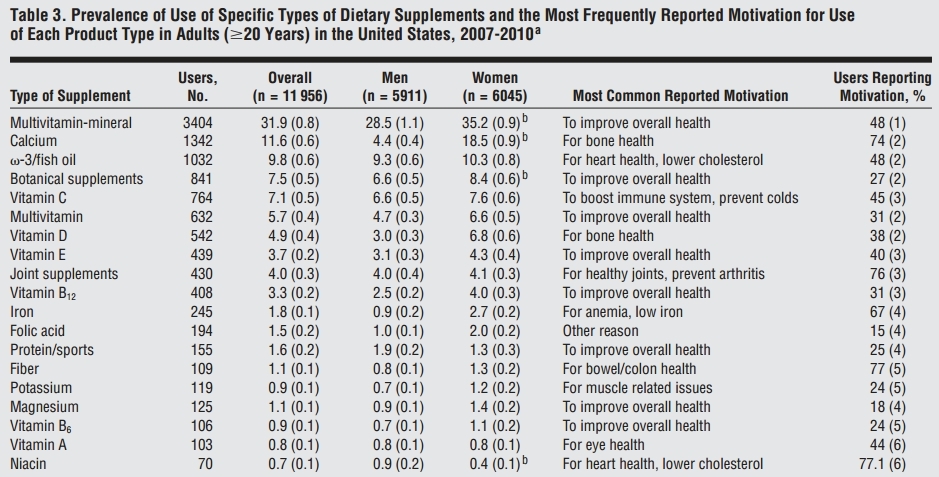
Table 2. Prevalence of Reported Motivations for Use of Dietary Supplements Among Adults ( 20 Years) by Sex in the United States, 2007-2010a,b
Abbreviations: NA, not applicable; SE, standard error.
a Data are presented as percentages (SE).
b These data are for nonpregnant females; pregnant women were excluded from this analysis.
c Indicates significant difference between sexes; P < .05.
d The relative standard error is at least 30%, but not higher than 40% and may be statistically unreliable.
The National Health and Nutrition Examination Survey guidelines recommend a relative standard error no higher than 30%.
The most common reasons that adults reported using dietary supplements were to "improve overall health" (45%) and to "maintain health" (33%) (Table 2). The next most common reason was for "bone health" (25%), and this was significantly more frequent among women (36%) than men (11%). Adults reported motivations for organ-specific health reasons less frequently than the motivations noted herein (eg, heart, joint, colon and bowel, skin, and eye health). Adults also reported using supplements to "to get more energy" (11%), for "mental health" (4%), and prostate health in men (4%) and for "weight loss" (3%) or "menopause or hot flashes" in women (2%). About 5% of adults also listed "other" as a reason for using dietary supplements. Some motivations differed by age (Figure). There was a significant inverse trend with age and a higher prevalence of reported use of dietary supplements to "improve overall health," "supplement the diet," "boost immunity or prevent colds," and to "get more energy" (Figure). There was a significant positive trend for supplement use with age and a higher prevalence of reported use of dietary supplements for site-specific reasons like heart, eye, and joint and bone.
Multivitamin-minerals (MVMs) were the most common type of dietary supplements reported (Table 3) and were used primarily to "maintain health" or to "supplement the diet." Calcium-containing supplements were the second most frequently reported product (12%) and were reported almost exclusively for "bone health" or for "healthy joints and prevention of arthritis." w-3 Fatty acids and fish oils were the third most frequently reported product and were used for various reasons, most commonly for "heart health or to lower cholesterol." Botanical supplements, multivitamins, vitamin E, vitamin B12, and protein-sports supplements were mainly used to "improve overall health." Vitamin D was used for "bone health"; about 4% used supplements categorized as "joint supplements" primarily for "joint health" (76%). Adults also reported that they used vitamin B12 supplements to "enhance energy" (25% overall; 21% in men and 27% for women).
Consumption of alcohol in the past year did not differ by use of any dietary supplement (Table 4). Non-users had a higher prevalence of 3 or more drinks per day than supplement users (23% vs 11%; P < .001), whereas supplement users were more likely to consume 1 drink per day (31% vs 19%; P < .001). Similar trends toward heavier alcohol use in nonusers of supplements were observed for the use of MVMs as well as botanical and herbal supplements. Overall, users ofdietarysupple-ments (any, MVMs, or botanical supplement) were more likely to report never smoking or former smoking than nonusers of supplements (Table 4). Users of dietary supplements and especially those using MVMs were more likely to report very good or excellent health than non-users.
About a quarter (23%) of the supplements were reported to be used on the advice of a health care professional. Multivitamin-minerals and calcium were the most frequently recommended products by health care providers (eFigure). The most common motivation for products recommended by health care providers were for "bone health" followed by "to improve overall health" (Table 5). Physicians and health care providers were more likely to encourage use of calcium supplements for women and for heart health for men.
Comment
Dietary supplements were used by about half of adults (49%) in 2007 to 2010, although this was slightly lower than in 2003 to 2006 (53%).3,12 Dietary supplements are defined by law as products that are intended to supplement the diet; they are not drugs and, therefore, are not intended to prevent, diagnose, treat, mitigate, or cure diseases. Our analysis indicates that the primary reasons for using dietary supplements in adults was to improve or maintain overall health, which may or may not include the prevention or treatment of disease. It is interesting to note that dietary supplements were reported to be used to "supplement the diet" in only 22% of users. Multivitamin-mineral products remained the most commonly reported type of supplement and were used primarily to improve health or maintain health.
As seen in this study and others, the use of dietary supplements is associated with lower BMIs, moderate alcohol use, more exercise, abstinence from smoking, and having health insurance. Previous research also suggests the supplement users have higher intakes of most vitamins and minerals from their food choices alone than nonusers.13,14
Figure.
Prevalence of reported motivations for use of dietary supplements among adults (>20 years) by age group in the United States, 2007 to 2010. Data are presented as percentages (standard errors [error bars]) for users of dietary supplements (n = 5514). *Significant difference between age groups; P< .05. The National Health and Nutrition Examination Survey guidelines recommend a relative standard error of 30% or less; all estimates were no higher than 30%. Improve indicates "to improve overall health"; prevent, "to prevent health problems"; maintain, "to maintain health"; supplement, "to supplement the diet"; immunity, "to boost the immune system or prevent colds"; energy, "to increase energy"; heart health, "for heart health or to lower cholesterol"; eye health, "for eye health"; joint health, "for healthy joints or arthritis"; and bone health, "for bone health."
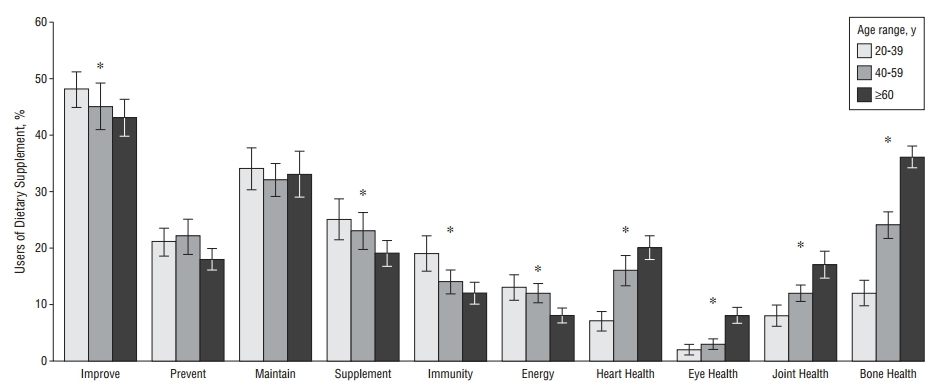
Table 3.
Prevalence of Use of Specific Types of Dietary Supplements and the Most Frequently Reported Motivation for Use of Each Product Type in Adults ( 20 Years) in the United States, 2007-2010a
a Data are presented as percentages (SE); the National Health and Nutrition Examination Survey guidelines recommend a relative standard error not higher than 30%, and all estimates were not higher than 30%.
b Indicates significant difference between sexes; P< .05.
State-of-the-Science Conference statement determined that, "the present evidence is insufficient to recommend either for or against the use of MVMs by the American public to prevent chronic disease."16(p256S) A recent meta-analysis examining the use of B vitamins to lower ho-mocysteine concentrations showed no significant effects at 5 years for cardiovascular events, cancer incidence, or all-cause mortality.17,18 Similarly, a meta-analysis examining antioxidant dietary supplements (vitamin E or beta carotene) showed that among the vitamin E trials
Table 4. Use of Alcohol in the Past Year, Cigarette Smoking, and Self-reported Health Among Users and Nonusers of Dietary Supplements in the United States, 2007-2010a
a Data are presented as percentages (SE). A user is someone who reported using a particular type of dietary supplement in the past 30 days, whereas a nonuser did not.
b Those who did not report consuming an alcoholic beverage in the past year were assigned 0 average drinks per day.
c Indicates significant difference between supplement use groups; P< .05. The National Health and Nutrition Examination Survey guidelines recommend a relative standard error no higher than 30%, and all estimates were no higher than 30%.
Table 5.
Common Reasons Provided for Use of Dietary Supplement Products Recommended by Healthcare Providers for Adults ( 20 Years) in the United States, 2007-2010a
a The National Health and Nutrition Examination Survey guidelines recommend a relative standard error no higher than 30%, and all estimates were no higher than 30%. Data are presented as mean(SE).
b Significant difference between sexes; P< .05.
there was no association between supplementation and prevention of cardiovascular disease or mortality, whereas the available beta carotene trials showed a small increase in all-cause or cardiovascular-related mortality.19 A Cochrane Review of 3 trials examining w-3 fatty acid supplementation showed no effect on the prevention of cognitive decline or incident dementia.20 Two recent metaanalyses have found supplementation with w-3 fatty acids (primarily from fish oils) to be of no or little value in preventing the risk of major cardiovascular disease events or all-cause mortality among heterogeneous groups of adults21 or in patients with a history of heart disease.22 In addition, 2 meta-analyses have reached different conclusions about the potential value of the dietary supplements glucosamine and chondroitin in delaying the radiologic progression (joint space narrowing) of osteoarthritis of the knee.23,24 Thus, the use of dietary supplements for health promotion is controversial not only because of a lack of sufficient research, but also because of conflicting evidence that is available from the existing research.
The questionnaire used to assess motivations was a finite list of potential motivations, and some disease states, such as cancer and obesity, were not specifically queried, although individuals could volunteer this information. A cancer diagnosis has been shown to serve as a motivating factor in initiating supplement use.25-27 Among cancer survivors,28 the top reasons cited for using dietary supplements included "the ability to help oneself"; "to boost the immune system"; "to provide more energy"; and "to help prevent cancer." Supplements are widely used not only by those recently diagnosed with cancer but also by longer-term survivors, with estimates ranging from 75% to 87%.29 A few other limitations of this research should be addressed; first, the NHANES is a cross-sectional study. While every attempt is made to ensure the participants are nationally representative and sample weights account for nonresponse and noncoverage, we cannot completely out rule that selection bias may occur.
Age and sex differences were evident in motivations for use. Older adults were more likely to use supplements for site-specific health reasons (eg, bone, heart, eye), whereas younger adults were more likely to use products with a short-term effect, such as enhanced energy or to boost immune function. Women were more likely to report use for bone health and men for heart health. However, men were also more likely to report use of products to improve and maintain health (vitamin D, botanical supplements, vitamin B12, w-3 and fish oils) or for mental health, whereas women were more likely to report use of products to enhance energy (vitamin B12 and vitamin B6) or for colon health (botanical supplements). Some products were associated with very specific reasons for use, such as calcium products for bone health, as evidenced by a high percentage of users reporting only 1 reason (Table 3). Other products were used for various reasons; for example, magnesium was most frequently used to improve health, but only by 18% of users— other frequent reasons for using magnesium were for heart health, colon health, bone health, muscle-related issues, or joint health. Thus, it seemed that some products were being used in many different ways by different people, making interpretation of motivations more complicated. Virtually no one used products for asthma, allergies, diabetes mellitus, to improve sleep, or to aid in relaxation despite several products being marketed for these purposes.
The motivations behind botanical supplement use have been studied more extensively than for other types of dietary supplements. In adults, use of herbs and botanical supplements has been related to being uninsured, using more prescription and over-the-counter medications, and for certain health conditions.30,31 National survey data find that most botanical supplement users do not report this information to their health care providers.30 This may be cause for concern because some botanical supplements have the potential to interact negatively with prescription medications. While some have suggested that botanical supplements are increasing in popularity to replace costly prescription medications,32,33 recent national data actually suggest a slight decrease in the use of botanical and herbal products.31
Americans spent more than $30 billion on dietary supplements in 2011.34 Our results indicate that adults often report supplement use to improve or maintain health; however, most products were used by personal choice (77%) rather than by the recommendation of a health care provider (23%). These data lend credence to the "inverse supplement hypothesis" that many supplement users are healthy individuals who want to take an active role in their own health, and who perceive supplements as a type of "insurance" against poor health.35
Very little is known about the efficacy of dietary supplements for disease prevention, management, or treatment in nutrient-replete populations. It is often difficult to study the use of supplements in disease prevention and health promotion in epidemiologic research, because supplement use cannot be disentangled from other health-seeking behaviors. Studying the use of supplements in randomized clinical trials is also difficult because they tend to be short in duration, whereas many of the chronic diseases of public health concern have a long latency period (ie, cancer, heart disease). Nevertheless, given the widespread use of dietary supplements for health promotion and maintenance, increased clinical research efforts are warranted to address safety and efficacy. Also, more investigation on the complex interplay of social, psychological, and economic determinants that motivate supplement choices are needed.36
Accepted for Publication: October 6, 2012.
Published Online: February 4, 2013. doi:10.1001 /jamainternmed.2013.2299
Correspondence: Regan L. Bailey, PhD, RD, Office of Dietary Supplements, NIH, Bethesda, 6100 Executive Blvd, 3B01, Bethesda, MD 20892-7517 ([email protected]).
Author Contributions: Study concept and design: Bailey and Gahche. Acquisition of data: Bailey and Gahche. Analysis and interpretation of data: Bailey, Gahche, Miller, Thomas, and Dwyer. Drafting of the manuscript: Bailey, Gahche, Miller, Thomas, and Dwyer. Critical revision of the manuscript for important intellectual content: Bailey, Gahche, Miller, Thomas, and Dwyer. Statistical analysis: Bailey and Gahche. Administrative, technical, and material support: Bailey, Miller, Thomas, and Dwyer. Conflict of Interest Disclosures: Dr Dwyer is a nonpaid public trustee of the International Life Sciences Institute, a 501(c) foundation that is funded by the food industry; holds common stock of approximately $10 000 to $15 000 in Bristol Myers Squibb, Merck, and Pfizer companies, which produce or have produced some dietary supplement products; and collaborated on the manuscript while serving as a senior nutrition scientist (consultant at the Office of Dietary Supplements, NIH). Funding/Support: This work was supported by the NIH, Office of Dietary Supplements.
Disclaimer: The findings and conclusions in this report are those of the author(s) and do not necessarily represent the views of the Office of Dietary Supplements or any other entity of the US Government. Online-Only Material: The eTable and eFigure are available at http://www.jamainternalmed.com.
References
Briefel RR, Johnson CL. Secular trends in dietary intake in the United States. Annu RevNutr. 2004;24:401-431.
Radimer K, Bindewald B, Hughes J, Ervin B, Swanson C, Picciano MF. Dietary supplement use by US adults: data from the National Health and Nutrition Examination Survey, 1999-2000. Am J Epidemiol. 2004;160(4):339-349.
Bailey RL, Gahche JJ, Lentino CV, et al. Dietary supplement use in the United States, 2003-2006. J Nutr. 2011;141(2):261-266.
Picciano MF, Dwyer JT, Radimer KL, et al. Dietary supplement use among infants, children, and adolescents in the United States, 1999-2002. Arch Pediatr AdolescMed. 2007;161(10):978-985.
Foote JA, Murphy SP, Wilkens LR, Hankin JH, Henderson BE, Kolonel LN. Factors associated with dietary supplement use among healthy adults of five ethnicities: the Multiethnic Cohort Study. Am J Epidemiol. 2003;157(10):888-897.
Rock CL. Multivitamin-multimineral supplements: who uses them? AmJClin Nutr. 2007;85(1):277S-279S.
Harrison RA, Holt D, Pattison DJ, Elton PJ. Are those in need taking dietary supplements? a survey of 21 923 adults. Br J Nutr. 2004;91(4):617-623.
TouvierM, Niravong M, Volatier JL, etal. Dietary patterns associated with vitamin/ mineral supplement use and smoking among women of the E3N-EPIC cohort. Eur J Clin Nutr. 2009;63(1):39-47.
Block G, Jensen CD, Norkus EP, etal. Usage patterns, health, and nutritional status of long-term multiple dietary supplement users: across-sectional study. Nutr J. 2007;6:30.
About the National Health and Nutrition Examination Survey. 2009. http://www .cdc.gov/nchs/nhanes/about_nhanes.htm. Accessed August 17, 2008.
National Health and Nutrition Examination Survey, 2007-2008 questionnaire files. http://www.cdc.gov/nchs/nhanes/nhanes2007-2008/DSQDOCE.htm#Interview _SettingandModeof_Administration. Accessed September 19,2011.
Gahche J, Bailey R, Burt V, etal. Dietary supplement use among US adults has increased since NHANES III (1988-1994). NCHS Data Brief. 2011;(61):1-8.
Bailey RL, Fulgoni VL III, Keast DR, Dwyer JT. Dietary supplement use is associated with higher intakes of minerals from food sources. Am J Clin Nutr. 2011; 94(5):1376-1381.
Bailey RL, Fulgoni VL 3rd, Keast DR, Dwyer JT. Examination of vitamin intakes among US adults by dietary supplement use. J Academy Nutrition Dietetics. 2012; 112(5):657-663, e4.
Rosenberg IH. Challenges and opportunities in the translation of the science of vitamins. Am J Clin Nutr. 2007;85(1):325S-327S.
National Institutes of Health State-of-the-Science Panel. National Institutes of Health State-of-the-Science Conference Statement: multivitamin/mineral supplements and chronic disease prevention. Am J Clin Nutr. 2007;85(1):257S-264S.
Clarke R, Halsey J, Bennett D, Lewington S. Homocysteine and vascular disease: review of published results of the homocysteine-lowering trials. J Inherit Metab Dis. 2011;34(1):83-91.
Clarke R, Halsey J, Lewington S, etal; B-Vitamin TreatmentTrialists' Collaboration. Effects of lowering homocysteine levels with B vitamins on cardiovascular disease, cancer, and cause-specific mortality: meta-analysis of 8 randomized trials involving 37 485 individuals. Arch Intern Med. 2010;170(18):1622-1631.
Vivekananthan DP, Penn MS, Sapp SK, Hsu A, Topol EJ. Use of antioxidant vitamins for the prevention of cardiovascular disease: meta-analysis of randomised trials. Lancet. 2003;361(9374):2017-2023.
Sydenham E, Dangour AD, Lim W-S. Omega 3 fatty acid for the prevention of cognitive decline and dementia [published online June 13, 2013]. Cochrane Database Syst Rev. doi:10.1002/14651858.CD005379.pub3.
Rizos EC, Ntzani EE, Bika E, Kostapanos MS, Elisaf MS. Association between omega-3 fatty acid supplementation and risk of major cardiovascular disease events: a systematic review and meta-analysis. JAMA. 2012;308(10):1024-1033.
Kwak SM, Myung SK, Lee YJ, Seo HG; Korean Meta-analysis Study Group. Efficacy of omega-3 fatty acid supplements (eicosapentaenoic acid and doco-sahexaenoicacid) in the secondary prevention of cardiovascular disease: a metaanalysis of randomized, double-blind, placebo-controlled trials. Arch Intern Med. 2012;172(9):686-694.
Lee YH, Woo JH, Choi SJ, Ji JD, Song GG. Effect of glucosamine orchondroitin sulfate on the osteoarthritis progression: a meta-analysis. Rheumatol Int. 2010;30(3):357-363.
Wandel S, Juni P, Tendal B, et al. Effects of glucosamine, chondroitin, or placebo in patients with osteoarthritis of hip or knee: network meta-analysis. BMJClini-calResearch. 2010;341:c4675. doi:10.1136/bmj.c4675.
Burstein HJ, Gelber S, Guadagnoli E, Weeks JC. Use of alternative medicine by women with early-stage breast cancer. N Engl J Med. 1999;340(22):1733-1739.
Lengacher CA, Bennett MP, Kip KE, et al. Frequency of use of complementary and alternative medicine in women with breast cancer. OncolNurs Forum. 2002; 29(10): 1445-1452.
Patterson RE, Neuhouser ML, Hedderson MM, Schwartz SM, Standish LJ, Bo-wen DJ. Changes in diet, physical activity, and supplement use among adults diagnosed with cancer. J Am Diet Assoc. 2003;103(3):323-328.
Ferrucci LM, McCorkle R, Smith T, Stein KD, Cartmel B. Factors related to the use of dietary supplements by cancer survivors. JAltern Complement Med. 2009; 15(6):673-680.
Velicer CM, Ulrich CM. Vitamin and mineral supplement use among US adults after cancer diagnosis: a systematic review. J Clin Oncol. 2008;26(4):665-673.
Gardiner P, Buettner C, Davis RB, Phillips RS, Kemper KJ. Factors and common conditions associated with adolescent dietary supplement use: an analysis of the National Health and Nutrition Examination Survey (NHANES). BMC Comple-mentAltern Med. 2008;8:9.
Wu CH, Wang CC, Kennedy J. Changes in herb and dietary supplement use in the US adult population: a comparison of the 2002 and 2007 National Health Interview Surveys. Clin Ther. 2011;33(11):1749-1758.
Pagan JA, Pauly MV. Access to conventional medical care and the use of complementary and alternative medicine. HealthAff (Millwood). 2005;24(1):255-262.
Su D, Li L. Trends in the use of complementary and alternative medicine in the United States: 2002-2007. J Health Care Poor Underserved. 2007;22:296-310.
Considering a post-DSHEA world. Nutrition Business Journal. 2012;17:1-9. http: //newhope360.com/site-files/newhope360.com/files/uploads/2012/10/TOC _SUMM120928.supp%20report%20FINAL%20standard.pdf.Accessed November 9, 2012.
Kirk S, Woodhouse A, Conner M. Beliefs, attitudes and behaviour in relation to supplement use in the UK Women's Cohort Study (UKWCS). Proc Nutr Soc. 1998;57:54A.
Conner M, Kirk SF, Cade JE, Barrett JH. Why do women use dietary supple-ments?The use of the theory of planned behaviour to explore beliefs about their use. SocSciMed. 2001;52(4):621-633.
--