Public health policies not keeping up with Vitamin D consensus
Arguing that vitamin D can help avoid bad COVID outcomes is widely dismissed as misinformation. Yet the latest results of the covidConsensus.org project tell a different story, says Daniele Fanelli (LSE) .
Calls to increase vitamin D levels to prevent bad COVID-19 outcomes have been ignored by policy makers and branded as misinformation by fact-checkers for over two years. And yet they are widely supported by published experts, according to a recent anonymous poll run on the covidConsensus.org platform. When does misinformation cease to be so? And are public policies keeping up?
Research suggesting that vitamin D deficiency might be an aggravating factor in respiratory infections predates the pandemic, but has been intensified by it. Since vitamin D is synthesised by exposure to sunlight and absorbed in fat tissues, the hypothesis would help explain a number of puzzling patterns about the virus, including the higher rates of hospitalisations and deaths among ethnic minorities, obese patients and generally wealthier (indoor-working) economies. The stakes are extremely high, because if vitamin D really had a protective role it would represent an exceptionally powerful public health weapon against COVID, since it can be produced and distributed cheaply and safely.
The main problem with the evidence surrounding vitamin D benefits is that such evidence was, and still is, mostly observational. In other words, it falls short of what is considered the gold standard of modern clinical medicine, represented by a Randomised Control Trial (RCT) that conclusively quantifies a significant causal effect. Consequently, several prominent medical bodies in the UK, for example the UK National Institute for Health and Care Excellence and the Royal College of Physicians, issued position statements in 2020 that acknowledged the promising nature of observational evidence. On the other hand, they emphasised the lack of conclusive evidence for a causal effect, and therefore did not recommend vitamin D as a prophylactic or therapeutic measure.
As circumstantial as it may be, however, the evidence seemed strong enough to other scientists, who have advocated for actively increasing the uptake of the vitamin in the population. One of the most prominent calls came from the vitaminDforAll.org initiative that issued an open letter early in 2021 calling for “immediate widespread increased vitamin D intakes” in the general population. The letter was signed by over 200 scientists and doctors, each of whom accompanied their signature by two numbers: the intake levels that they recommended, and those that they followed personally. Most recommend taking 4000 IU (International Units), and they personally take much more.
The response of public health policymakers has been tepid, if there has been one at all. In the UK, the NHS ran a programme to supply 400 IU of vitamin D to extremely vulnerable patients, which operated for a few months during last winter and which has now been scrapped. No similar programme was even attempted in the US, at least at the national level, despite the fact that the National Institute of Allergy and Infectious Diseases director Anthony Fauci reported taking Vitamin D supplements – apparently at a dosage of 6000 IU, as he wrote in a private email.
Presumably on the basis of these official positions, the vitamin D issue has been taken to be a prominent example of health disinformation. While websites that recommend increasing vitamin D levels abound, an equally large number of reputable sources “debunk” the idea. It certainly didn’t help the vitamin D cause that one of the earliest and most widely circulated studies reporting its benefits turned out to be a complete fabrication. Still, one might question whether current evidence is sufficient to state that 85% of YouTube videos on the subject suggested a preventive effect, and therefore qualify as “misleading”, as a recent content analysis on COVID-19 and vitamin D misinformation on YouTube states (to be published in JMIR Infodemiology).
But the vitamin D advocates are unrelenting. Promising studies and reviews have kept appearing in the literature, and new open letters have been issued, including by the Academy of Medicine of Turin.
So where does the scientific consensus lie on vitamin D? A few weeks ago, the covidConsensus.org project sought to find out.
This project started a year ago as an attempt to assess the level of scientific consensus on controversial questions surrounding the pandemic and disseminate a more nuanced public understanding of scientific debates. It works as follows: for any topic of interest, a suitable question is crafted and relevant articles are searched and retrieved from the peer-reviewed literature using a combination of keywords. The email addresses of the corresponding authors are retrieved, and they are sent an invitation email containing a secret key. The key grants them the exclusive ability to cast a vote on the question, add a single post explaining their reasoning, and to comment on any other post, all entirely anonymously. Unlike ordinary surveys, authors can change their opinion and shift their vote whenever they like, and the website keeps track. The first results of this project were presented one year ago on the LSE COVID-19 blog.
A total of 865 corresponding authors of peer-reviewed articles discussing vitamin D and COVID were invited to express on the “vitaminForAll” call mentioned above. The response received was remarkable, both for its volume and for the level of consensus expressed. At the time of writing, circa 16 percent of all invited authors have voted (Figure 1). This is a higher response rate than any of the four previous questions asked by the project.
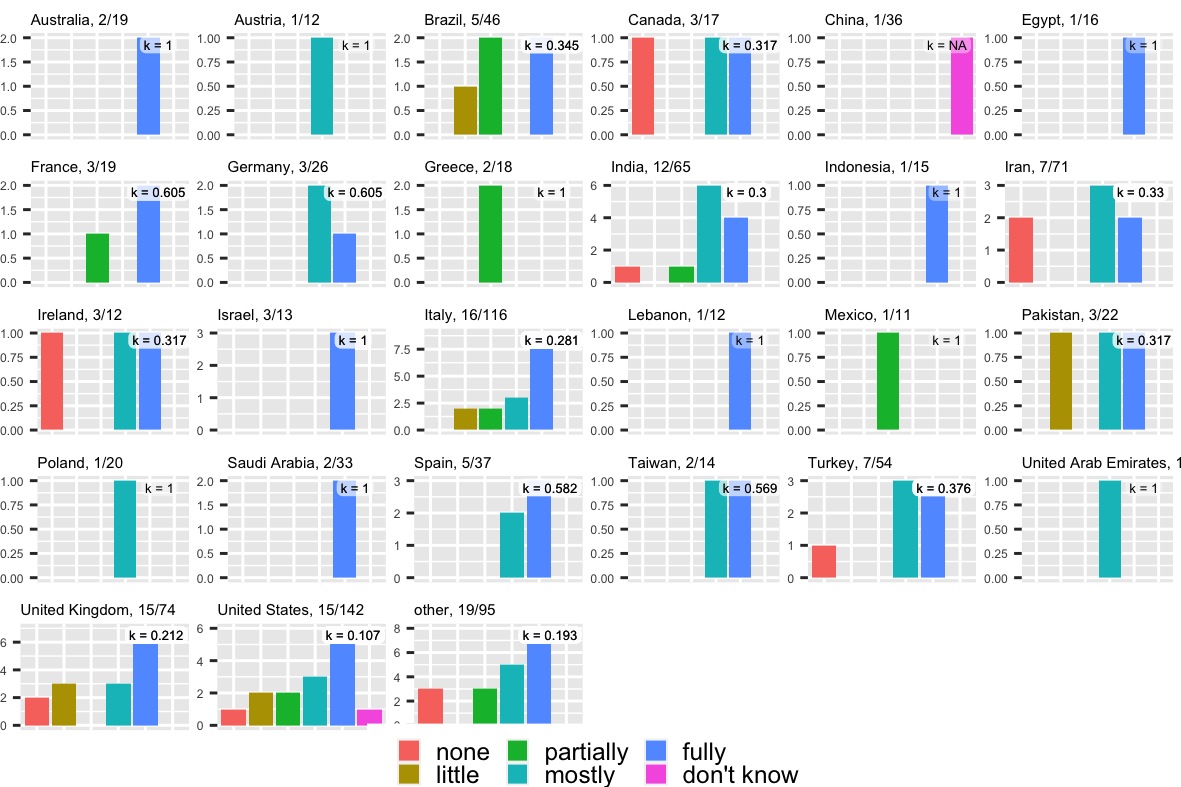
Figure 1: Distribution of agreements with the vitaminDforAll statement
As shown in Figure 1, over 72 percent of authors who responded “mostly” or “fully” agrees with the call to increase vitamin D uptakes to combat COVID. Remarkably, the measured consensus is similar across categories of respondents. Unlike what was previously observed, for example, within patterns of consensus towards lockdown policies, there is no significant difference in the rate of agreement for authors of different countries, disciplines, or genders. As usual, a full breakdown of the data can be found on the project’s webpage.
Even more striking, the level of consensus has remained virtually constant over time, as votes have accumulated over several days. In addition to casting their votes, participating authors have shared extensive explanations for their reasoning, and have included numerous references to the scientific literature that motivated their position. These articles will all be collected in the associated “current evidence page”.
These results constitute the strongest evidence of a scientific consensus that this project has measured to date. The distribution of support follows a natural descending curve (Figure 1), heavily skewed towards agreement, with a small uptick of “strongly disagreeing” opinions.
The dissenting opinions appear to be primarily by experts publishing in the field of clinical medicine, and their scepticism verges primarily on the observational nature of existing evidence. A clinical medicine author who voted “none”, for example, argued that “there is sufficient data justifying an association of low D with increased COVID-19 risks, but insufficient interventional data from well-designed clinical trials to support population-based recommendations to increase D”. Another one who voted “little” explained that “vitamin D increases from sun exposure have definitively correlated with improved outcomes. We do not make clinical decisions based on observational studies.” To comments like these, other authors have offered counter arguments – for example, one author countered that the unquestioned use of vitamin C today to prevent scurvy is based on a 17th century observational study that has never been subject to a randomised trial.
Therefore, the terms of the debate on Covidconsenus.org mirror those in the scientific literature: both sides acknowledge the nature of existing evidence, but have differing views on how conclusively it supports a public health intervention. However, to the extent that the scientific consensus is measured in these results, it shows clear and broad support among the research community for adopting vitamin D supplementation as a measure against COVID.
While systematic biases in these results are possible, they are less likely in these results than others. A 16 percent response rate, while not ideal, is comparable or indeed superior to that of many online surveys currently published (for example, a highly cited survey on the “unequal effects” of the pandemic on scientists, which was published in the prestigious Nature Human Behaviour, had a modest 1.6% response rate). Notably, whilst respondents have the option to answer “don’t know”, very few do so. This suggests that non-respondents are likely to be authors without an informed opinion, whereas those that do answer have informed reasons to do so. Indeed, the numerous literature references that voting participants cited in their comments corroborate the impression that they have well-formed opinions that they wish to share. The homogeneity of positions across categories and time should further raise confidence that results are free from systematic biases.
It could still be the case that the probability of responding to the invitation is directly correlated to the level of agreement with the statement, giving rise to an “agreement bias”. But why should that bias be more likely than the reverse? Indeed, in previous controversial questions asked by the site, very high levels of consensus were registered against the controversy and in support of the official position, for example on the origins of COVID or the risk of vaccine escape mutants.
The findings raise questions about how well current policies reflect the scientific consensus. In the most optimistic scenario, the scientific consensus has shifted only recently, and policymakers will revise their positions to take the mounting consensus into account.
Critics might fairly maintain that science does not progress by vote counting: even when expressed by the majority of experts, a belief might be wrong. In the issue at hand, this would entail that the proponents of RCTs are correct, and policy makers should stick to their official gold standards. But if this is the case, then in what sense can we trust that public health policies, or indeed the very concept of “misinformation”, reflect the current scientific consensus? And if the majority opinion of peer-reviewed published authors does not reflect the current scientific consensus, then what does?
This post represents the views of the author and not those of the COVID-19 blog, nor LSE.
Daniele Fanelli

Daniele Fanelli is an LSE Fellow in Quantitative Methodology at LSE. He is a member of the Research Ethics and Bioethics Advisory Committee of Italy’s National Research Council, for which he developed the first research integrity guidelines, and of the Research Integrity Committee of the Luxembourg Agency for Research Integrity.
Votes by country: mamy fully agree, (only 134 votes out of 888 requests)
Many comments
Example - Dr. Grant
185, Wednesday, 26-Jan-22 22:10:18 UTC, clinical medicine, voting: fully
Yes. My publication has over 1000 citations: Grant WB, Lahore H, McDonnell SL, Baggerly CA, French CB, Aliano JA, Bhattoa HP. Evidence that vitamin D supplementation could reduce risk of influenza and COVID-19 infections and deaths. Nutrients 2 April 2020, 12, 988. https://www.mdpi.com/2072-6643/12/4/988 Supported by this recent article: Association of Vitamin D Status and COVID-19-Related Hospitalization and Mortality. Seal KH, Bertenthal D, Carey E, Grunfeld C, Bikle DD, Lu CM.J Gen Intern Med. 2022 Jan 1:1-9. doi: 10.1007/s11606-021-07170-0. There are many diseases for which vitamin D reduces risk including cancer, cardiovascular disease, diabetes, other infectious diseases, etc. and all-cause mortality rate. The medical systems say they want to see successful vitamin D RCTs. RCTs have seldom supported the role of vitamin D in reducing risk of disease since they have been based on vitamin D dose (often low) rather than achieved vitamin D level: Critical Appraisal of Large Vitamin D Randomized Controlled Trials. Pilz S, Trummer C, Theiler-Schwetz V, Grübler MR, Verheyen ND, Odler B, Karras SN, Zittermann A, März W.Nutrients. 2022 Jan 12;14(2):303. doi: 10.3390/nu14020303. However, at least the U.S. health care system does not want vitamin D to be accepted since they obtain income and profit through treating disease, not preventing it. Thus, the demand for vitamin D RCTs is used as a roadblock to the acceptance of vitamin D. There are many vitamin D papers supporting vitamin D at pubmed.gov, scholar.google.com, Vitamin D Life.com, and Grassrootshealth.net