Off topic: Low-income black churches interest in early disease detection
Article below is from Salon – Sept 2013
Wonder if churches might increase vitamin D usage in those with dark skin.
FACT: Most people with dark skins and modern life style have low vitamin D.
FACT: Vitamin D levels in the Southern US have dropped a lot in past 40 years with the use of air conditioning, increasing the problem
FACT: Increasing vitamin D improves health
Note: Poor health of dark skinned immigrants is a big problem around the world - churches might be able to help
See also Vitamin D Life
US coalition of Black and Latino churches hope to reduce the 3X COVID-19 disparity - Aug 2021
Immigrants and refugees had lower vitamin D levels – Jan 2013
88 percent of African immigrants to Melborne had less than 20 ng of vitamin D
Most immigrant women in Sweden had little vitamin D and lots of muscle pain – May 2013
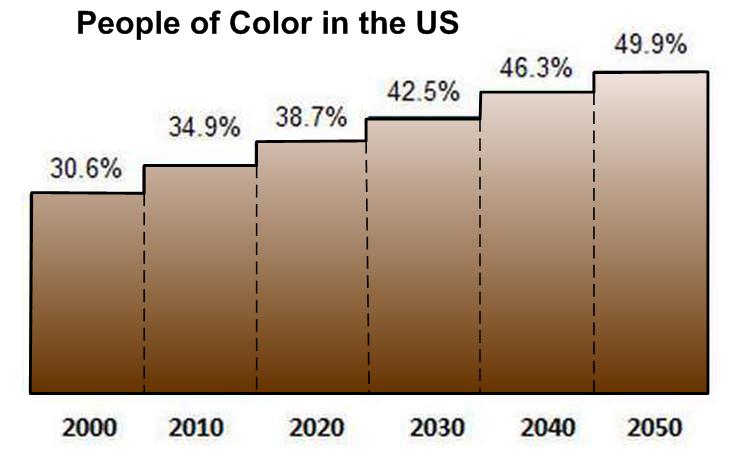
Half of the US will be people of color – wonder how many will be vitamin D deficient which has the following chart
Possible options for churches around the world include
Education about the benefits of vitamin D (in a way and language that the people can relate to)
Provide vitamin D at little or no cost.
The following does not include graphics or links
It really does take a village: How Memphis is fixing healthcare
One hospital and hundreds of churches race to heal America's most impoverished city -- and save money too
By Alex Halperin
“First and foremost, I give honor to God.”
Carole Dickens, a registered nurse, stood before the black congregation at Lakeview Community Temple in Memphis, Tenn., urging them to get a mammogram. Anyone who’s uninsured, she said, might be eligible for a free screening.
“African-American women do not have breast cancer as often, as prevalent, as Caucasian or white women,” she said. But, “we are so late going for an early detection that by the time we get there, it is at a stage that your prognosis is really, really poor.”
“You don’t want anybody to know your business? You will be dead and everybody will know it.”
Dickens, who has light brown skin and wavy silver hair, told her audience that she also belongs to a Church of God in Christ church, a predominantly black Pentecostal denomination with Memphis roots. After she spoke, she passed around a form and women began signing up.
The pastor approached the pulpit and affirmed Dickens’ message. “When we get through dancin’, and we get through shoutin’, we still have to live.”
Preventing and treating chronic disease for low-income patients is one of the most vexing and expensive public health problems in this country. Factors like poor diet and education, distrust of authorities and lack of access to primary care contribute to high rates of conditions that, once they arise, require decades of care.
We can’t calculate the cost in joy and fulfillment of premature death and disease. And the financial toll approaches similarly metaphysical heights. In 2011, taxpayers covered an estimated $414 billion in spending on Medicaid, the government health program for low-income Americans. That price tag excludes direct and indirect including major portions of care for low-income veterans and seniors.
In the middle of the last decade, Methodist Le Bonheur Healthcare, Memphis’s largest hospital system, began teaming up with churches to address the city’s abysmal health situation and reduce the cost of care. This collaboration has grown into the Congregational Health Network, which has received attention in national public health circles, and from the Obama administration, for reducing the costs of care and improving outcomes for low-income patients. The Memphis method offers lessons to hospitals nationwide wrestling with similar problems. But successfully replicating the program will depend on hospitals’ ability to rethink their function in the communities they serve. Could the answer really be as simple as a woman testifying in church about the importance of mammograms?
As the pastor preached, Dickens, the nurse, and Dorothy Seawood, her point woman at the church, stepped outside to talk shop. They made plans, and caught up on news, but the conversation kept returning to their mission: how to engage congregation members in their own health.
“People don’t want you to know they’ve got high blood pressure ,” Dickens said. “It’s already a silent killer. By the time they go and get the test to even identify, they’re at stage four.”
“A lot of people think that when God heals he don’t send a doctor,” Seawood, whose pure white outfit indicated her status as church missionary, said. “He does it that way sometimes, with the laying on of hands or by your faith. But God also has doctors out there. He’s also got nurses out there. He’s also got medication out there. I thank God for all of it. Some people think it ain’t God.”
“A whole lot of it is misinterpretation of scripture,” Dickens said.
“They don’t want anybody to know that they’re taking pills,” as if, she added, “that’s a signal that ‘I’m not trusting God.’”
“I can’t understand,” Seawood said. “When you say we have food to give away, there’ll be a line down the street.”
“That’s right.”
“For a medical exam …”
“You can’t get them there.”
“You can’t get them there.”
CHN director Bobby Baker addresses an audience. Courtesy of Methodist Le Bonheur Healthcare
Memphis isn’t the first city you’d expect to solve a national public health crisis. Census data found it the poorest metropolitan area in the country.
Tennessee’s governor recently called his state one of the “least healthy” in the nation and Memphis is unhealthy even by Tennessee’s standards.*
The false promises of the post-Jim Crow South live on in the city’s health disparities. According to recent statistics, the infant mortality rate for Black Memphians is 13 per 1,000 live births, compared to four for whites. Black Memphians with diabetes are more than three times as likely as non-black diabetics to have a leg amputated due to complications from their disease.
Teresa Cutts, who is in charge of evaluating the Congregational Health Network, calls Memphis the “urban hub of delta poverty” and describes the majority black city’s rate of obesity, diabetes, congestive heart failure, kidney disease and hypertension as a “chronic co-morbidity cocktail.”
The CHN began to grow into its current form in 2005 when Methodist hired Gary Gunderson, a scholar with a doctorate in ministry, who had made a career studying the confluence of faith and health. In 1997 he wrote that “the root health problem is alienation and meaninglessness,” arguing in effect that faith and health are inseparable. He thinks about health, he said in an interview, “more as a social movement than an assembly of services people need when they get sick.”
Hospitals and churches both receive us at times of vulnerability and weakness, but medicine and religion are not always easy allies. Hospitals heal bodies, while churches aspire to something more abstract. Hospitals, Gunderson said, generally function by homing in on a patient’s condition. He wanted Methodist to better understand who and what else patients could access outside the hospital that might contribute to their health.
Before coming to Memphis, Gunderson had directed the Interfaith Health Program at the Rollins School of Public Health in Atlanta. While there, he worked with communities in Africa to identify local health resources in a process called “asset mapping.” An asset might be tangible, like a local charity, or ephemeral, like prayer.
Memphis was the first place in the U.S. where he applied this idea. In 2007, he told Memphis Medical News that the city is “a community in which the health challenges are so deeply rooted in the social fabric that it requires a lot of faith to engage.”
When Gunderson arrived at Methodist, “Dialysis clinics were then popping up all over our community,” Bobby Baker, CHN’s director, said. “We were seeing dialysis patients in their early 20s.” Some hospitals, would have begun with a small pilot program. But, Baker explained, the city’s needs were too urgent. “We’re trying to elevate the level of health in the community,” he said. “We’ve got egregious poverty, income disparities, heart disease, and diabetes.” To Baker and the leaders at Methodist, only a more ambitious campaign could make a difference.
From a financial perspective, a sweeping measure made sense as well. At the time, Methodist was treating sick patients instead of preventing illness; this is to say, it was acting a lot like a hospital. But Methodist’s leaders had an incentive to change. As a major provider of indigent healthcare, the hospital could choose between mitigating illness or waiting to provide expensive, often unreimbursed care later. “It was a “pretty straightforward economic case,” Methodist CEO Gary Shorb said.
Gunderson’s “asset map” concept may sound a little airy, but when applied to Memphis a valuable alignment of resources reveals itself. One asset is Methodist, a faith-based hospital system with facilities around the metropolitan region. Memphis also boasts roughly twice as many churches per capita as New York and Chicago, and religious life has long been central to African-American life in the city. Memphians also appear to be devout. A Methodist survey in 2006 found that 70 percent of patients with outstanding bills said they had been to church in the past month.
To succeed, Methodist has to overcome a long-standing distrust of the medical establishment within the black community. During the infamous Tuskegee experiment, doctors withheld treatment from poor, black men infected with syphilis for decades to observe how the disease ravaged and killed the men. The program ended in 1972. One of Tuskegee’s enduring legacies, I heard repeatedly, is that aspects of medicine that suggest research or withheld care, such as hospice, are particularly fraught subjects in the black community. Memphis, where hospitals were segregated, for both doctors and patients, within the living memory of seniors now entering intensive years of medical care, is not well positioned to overcome these historic wrongs.
“We’re trying to integrate two worlds,” Cutts said. An alliance, then, between a large hospital and the city’s primary black power structure could only move at the “speed of trust.” In his 1997 book, “Deeply Woven Roots,” Gunderson argued that church congregations are uniquely capable of bridging rifts like this one:
In general, collaboration depends on people comfortable enough in their own worldview that they do not fear differences. The congregation is the place where such risk taking faith is formed and reinforced … It is easy for utilitarian collaborations to run roughshod over the source of enduring community connection. This happens when houses of worship are viewed as mere delivery points for health interventions or, conversely, when public health agencies [or hospitals] are viewed as mere funding agents to support church programs. A little perspective could help here. If a religious tradition has survived for 3,000 years it deserves credit for its insight into how the world works. On the other hand, for 2,900 of those years we were generally satisfied with a life expectancy of less than 50 years. Public health science deserves most of the credit for extending that to 75 years in the last century. Maybe health scientists know something too.
The hospital convened a group of 12 area pastors and asked them to collaborate on a document, now called the “covenant,” that would serve as a framework for a partnership. Together, the churches and hospital system would create what Baker, the CHN director, called a “web of trust.”
For a document addressing matters as portentous as health and faith, the covenant reads like a bland memo. Its achievement is avoiding the implication that the hospital is taking advantage of the partner churches. “We’re very intentional about not using hospital language, very intentional using the language of the clergy, using the language of the congregations, because this was not a hospital program. It’s a community program,” Baker, an imposing bald man who dresses in pinstripe suits, said. The process of writing the one-page document collaboratively lasted about six months, Baker said. As a pastor explained to Baker, “‘I’m a shepherd. I’ve got to be careful how I lead my sheep.”
The pastors finished the Covenant in 2006, and since then more than 500 churches have signed the document. Most, but not all, of these congregations are predominantly African-American.
Here’s how the Congregational Health Network functions: The director oversees 10 navigators who have training in fields like nursing and community organizing. (Carole Dickens, who told the church about mammograms, is a navigator.) One or two unpaid volunteers at each church serve as ”liaisons” and work with navigators to promote healthy living in the congregation and work with anyone who’s sick.
When a patient in the network arrives at the hospital, she shows a card identifying her as a CHN member. Just as an insurance card activates monetary resources, the card activates her social safety net. Her church liaison is notified and her fellow congregants commit to support her by making hospital visits and praying for her recovery.
But CHN relies on more than just the power of prayer. Before the hospital discharges a CHN patient, she’ll discuss her situation with a navigator or liaison. Does she understand her drug regimen? Will she need help with cooking or cleaning? Does she have a way to get to church, the doctor or the pharmacy? Would she like a daily phone call or to have conversations about spiritual concerns? By determining a patient’s needs, the liaison can then facilitate her recovery.
More than 16,000 people have signed up for CHN, but the hospital believes the network reaches far wider. People who register up tend to be older, active churchgoers who are “planning to get sick,” one Methodist employee explained. But the member churches estimated 200,000 members could access CHN’s benefits if they suddenly need them.
The liaisons are typically older women confronting the same chronic conditions as congregants. This commonality of experience doubtless creates a comfort between patient and liaison that an unfamiliar nurse hired by the hospital would struggle to match. In an email Gunderson wrote, “I think that CHN is more about the liaisons and thus more about the women of the church than it is about the mostly male clergy. Clergy are crucial for their overall leadership and power, but I think it is the liaisons that are moving the data.”
The data is impressive. Methodist says that CHN members, many of whom are living with chronic diseases, are staying in the hospital for less time since they enrolled and the cost of caring for the same patients has fallen since they joined the network. A study of CHN patients showed that after discharge, a group of them stayed out of the hospital for a median of 426 days compared with 306 days for patients not in the network, an improvement of almost 40 percent—hospital administrators are watching readmissions data closely because the Affordable Care Act penalizes hospitals when patients are readmitted within 30 days. Over a three-year period, CHN members also had a significantly lower mortality rate. Methodist says CHN costs it about $1 million per year to run, not including outside grants, and saves the hospital $4 million in annual costs.
Dr. Karen Joynt, a cardiologist and instructor in health policy at the Harvard School of Public Health, hadn’t heard of the Memphis model, but the data rang true to her. Readmissions are “affected by patient engagement, and affected by access to outpatient care, and those are all things that, particularly in poor and minority communities, are just a lot more complicated,” she said. Compared with affluent suburbanites, such patients are more likely to have concerns beyond following doctors’ orders. They may be a primary caregiver for a child, lack access to outpatient care or, due to a cognitive impairment, may be unable to follow medication regimens of up to 20 pills a day. “Health is only kind of about healthcare,” Joynt said. “It’s a lot about what happens outside the hospital.”
“This is one of the iconic successes around the country,” said Thomas Cannell who studied the CHN and is developing a similar, though so far much smaller, program for New York City’s health department. As a secular system, all kinds of community organizations can join, but so far, he said, all of the nine member groups are churches.
Echoing Gunderson, Cannell described Methodist’s program as a version of “patient-centered healthcare,” an important trend in clinical medicine. The idea is to see patients as more than an “interesting kidney,” and instead create “systems that build on all those assets that are already in their lives.”
Many urban hospitals have community outreach programs. Methodist’s most impressive accomplishment, Gunderson said, is “to hold the trust of hundreds of congregations in a city as traumatized as Memphis.” If hospitals nationwide could replicate CHN’s results, they would restore countless years of healthy life. They would also save billions of dollars.
A girl gets a dental exam at a health fair in Memphis. Courtesy of Methodist Le Bonheur Healthcare
The ZIP code 38109 forms a crude triangle at the southwest tip of Tennessee, wedged between Mississippi and the Mississippi River. Forty-six thousand people live there; almost all are black and more than 28 percent live below the poverty line.
In early August, Methodist hosted a health fair at a community center gym in 38109’s Riverview-Kansas neighborhood. A DJ blasted party anthems as visitors sat for blood sugar, cholesterol and blood pressure tests and received individual consultations. A national pharmacy chain distributed pamphlets on childcare and coupons for essential items. Walking around the perimeter, a visitor could grab a meager packet of school supplies, find information on free birth control, and score a stress ball; boys started throwing them around the room and launching them at baskets.
Outside, at regular intervals, boards covered the windows of the area’s solid brick bungalows. Buildings that had once been stores looked like they had been burned or allowed to collapse. The gray muggy afternoon contributed to the gloom. Someone had painted “If you are not spending money do not enter store” on the wall of a “grocery” near the community center. In this neighborhood, “The closest you’ll get to a fresh fruit or vegetable might be a potato,” a navigator said. No such luck. But the store did stock individually packaged pickles. Earlier this year, Memphis’ superintendent recommended closing the nearest high school due to gang activity and financial concerns, a move that would yank away another potentially stabilizing element. Elvis Presley Boulevard runs one mile to the east and the major thoroughfare is so saturated with fast food restaurants that one Methodist doctor calls it heart attack row.
After a few days in Memphis, I had lunch with Bobby Baker and the pastors of two CHN member churches in southwest Memphis, Eric Winston and James Kendrick. After grace, we dug into beef lasagna, salads and pork chops in a private hospital dining room. The pastors good-naturedly one-upped each other with parables and quotations from scripture before they turned to their congregations’ health.
“Doctors, I think, enjoy being doctors. And so they will flaunt their medical expertise in light of the lay people who don’t understand,” Winston said. He sometimes sits in his parishioners’ hospital rooms, serving as a mediator. After the doctor speaks, Winston said he might ask the patient, “Did you understand what Dr. So and So said?’ and they’ll say, ‘Pastor, I really don’t,’ and I’ll say, ‘Doc, why don’t you ex-plain it again so she’ll know her prognosis.” (One experienced chaplain said it’s not unusual for a doctor to tell a family that their relative has died and they don’t get it until the chaplain rephrases the news.)
Pastor Kendrick saw a teachable moment in his experience with prostate cancer, “One thing that happened to me when I was diagnosed was I told the congregation. The Lord spoke to me: ‘These folk trust you with everything they go through and now here you are. What are you gonna do?’ So I stood up and I told them.”
“I said, ‘You’re going to see some weight loss.’ I explained some things to them. I said, ‘I’m going to do some things differently,’” he continued. “They’re watching all of this. Watching you on a regular basis. Many of them were wondering, ‘Are you OK?’ And I would talk to them every Sunday.”
“That kind of transparency is necessary from the pulpit to the people,” Winston picked up. “Since I told them I have diabetes … when we have these pot luck dinners they say, ‘Pastor, this is peach cobbler made with Splenda and we did this just for you.’ And I say, ‘Well, thank you. The carbs are still high but give me a little piece.’”
“In the past we haven’t talked about [sickness] publicly. Everything was so silent and taboo,” Winston continued. “Christian people get sick. Pastors catch cold. Those kind of things happen and we have to be real with people if we expect them to be real with us.”
Kendrick agreed. “I just talked to a pastor six months ago who was sharing with me just outright, ‘If something’s wrong, if something’s happening with me, I don’t tell ‘em. They don’t need to know.’ And I was like, ‘You can’t do that. How do you expect to change your people to get them to where they need to be … How will the story ever really change?’”
“Healing is telling the story,” Winston said. “It’s biblical, James 5, ‘If any man has faults, confess your faults, one to another that you might be healed.’”
“So many of our people they just don’t believe things can be any different,” Kendrick said. “And that’s why we’re doing some of the stuff we’re doing.”
Progress can be slow. Winston remembered men telling him, “Pastor I’ve never had the finger.’ And what they mean is that they’ve never had the doctor stick their finger in their …” he searched for the word, “behind, and check the prostate. ‘But I’m going.’ See, that’s a breakthrough moment for a lot of guys.
“Or when a young mother said, ‘I learned how to check for lumps in my breast,’ his voice got high. “And they don’t mind talking to you about it. Or when my mother stands up in church and says, ‘I’ve had a mastectomy, I know I look good but something is missing … And I’m no less woman.’”
“That’s changing the story,” Baker said. “The story is that you have a mastectomy or hysterectomy and that makes you less of a woman. And here is this mother standing up in church changing the story.”
Pastor Eric L. Winston at his church in Memphis. Courtesy of the Mt. Zion Baptist Church.
Russell Belisle, a CHN navigator, is a large man with a goatee and a lumbering gait. A longtime chaplain and pastor, he possesses an almost charismatic patience, as if he can calm the molecules in the air. When Belisle visits patients in their rooms, he prefers to sit down next to their bed. By bringing himself to their level, he embodies CHN’s thinking.
As Belisle rounds in the hospital, he looks for clues about the patients’ health. He pays attention to what’s in their IV bags and how aware patients are of their condition. He discreetly notes if they have two legs, and looks for flowers, balloons and cards to see if a patient has had guests. “I’m looking for that connection,” he said. “Can I connect with that person who connects with you? And how are we going to work together to take care of you?”
He’s also a patient advocate. A woman with no teeth shouldn’t have a plate of solid food. A patient whose door sign says she can’t eat or drink shouldn’t be whaling on a BBQ pork sandwich. Belisle told her to enjoy the sandwich, and then notified someone in the hall.
As a navigator, Belisle asks patients if there’s anything he can do. One woman complained and he let her. When patients ask him to pray with them, he leads them in prayer. In these gestures Belisle doesn’t individually restore people to health. But his efforts to monitor and support patients month after month contribute to CHN’s progress.
Following him for an afternoon, I couldn’t evaluate the results of his work; measuring the entire CHN’s impact presents an exponentially greater challenge. The Department of Health and Human Services’ Agency for Healthcare Research and Quality rated the strength of Methodist’s data “moderate.” In essence, this means that the success seen in CHN patients might not be caused by the network itself. Research shows that people with strong social support networks are healthier, so going to church, rather than the CHN’s features, could be the variable improving congregant health.
Methodist’s Teresa Cutts, who directs evaluation of CHN, explained some challenges of interpreting the CHN’s results. “Data bias is definitely a problem. Those that register [for the network] do self-select, even from the congregations, so that is a factor.” However, she added, in Memphis so many people seem to go to church that attendance alone cannot account for the improvement.
Another question is whether CHN’s success can be replicated elsewhere. Methodist did not invent the idea of offering patients emotional and logistic support. Community health workers save lives all over the world. CHN’s contribution may be how well it fits Memphis.
“Memphis itself may be a unique setting,” Dr. Owen Phillips, an OB/GYN and a professor at the University of Tennessee’s medical school in Memphis, said. “African-American churches have very strong leadership in play and if the pastors say, ‘We’re going to do this,’ people do it”
“The real debate about community health workers is how are you going to recruit ‘em and how are you going to pay ‘em?” Phillips, who’s studying CHN, said. In Memphis, “They’re doing it for Jesus, for the greater good … Where are you going to tap into that spirit if not in a faith-based initiative?”
Cutts doesn’t believe paying the liaisons is the right approach. She pointed out the corollary that a hospital that pays community health workers can also lay them off. “If someone does something for love and not money, you decrease the incentive if you start to pay them,” she said.
Four Detroit hospitals have developed an initiative inspired by CHN to address maternal health and infant mortality. Dr. Kimberlydawn Wisdom, chief wellness officer of the Henry Ford Health System in Detroit, called Methodist’s project a “beautiful natural fit” for Memphis.
“You don’t have to pay a church to care,” Gary Gunderson said. A major difference between the Detroit and Memphis programs is that the latter relies heavily on unpaid volunteers who, by not being paid, “created a huge cloud of caring.” In Detroit, they’ll see if paying people can work as well.
CHN’s most significant contribution may be demonstrating that a hospital adapting to and communicating with a complex patient community can make change. Detroit debt to the CHN is not seen in producing an exact replica, but by understanding that its project must meet its patients in their own communities. The program includes a social media element to reach young adults since they congregate on Facebook and Twitter instead of at church.
Last year Wake Forest University’s hospital system in Winston-Salem, N.C., hired Gunderson away from Memphis to build a program like the CHN. In North Carolina, Gunderson will be adjusting the model to a new community.
“I don’t think you need Deep South delta religion for this to work,” Gunderson said. His new employer seems to agree. Wake Forest didn’t hire him, he said, “because they want North Carolinians to pray better.”
At a health fair. Courtesy of Methodist Le Bonheur Healthcare
“We’ve only recently come to believe that Descartes and Plato are right: that you can take a human being and separate them into a body and a spirit and put the body on one side and say it’s the purview of science and medicine and put the spirit on the other and say it’s OK for the church to mess around with your spirit,” Dr. Scott Morris, a Memphis physician and minister, said. “That to me is a fundamental flaw.”
Regardless of what forces you see at work, CHN’s personalized approach has generated excitement about how to better care for very sick patients. But even if the most promising CHN data holds up, the network has far more to accomplish in Memphis. In all likelihood, the city will continue to see its healthcare disparities for years to come. And so far the savings are insignificant for a sprawling urban medical center like Methodist with more than 11,000 employees.
Morris founded the Church Health Center, one of CHN’s partner clinics, in 1987. It focuses on treating the working uninsured. Years later he recommended Gary Gunderson to Methodist. One morning, in his cluttered office, he assessed CHN’s progress and future:
“You’re not throwing rocks at me if you tell me some of this feels very soft. I totally get it. But it’s not going to stay soft,” he said. “The Affordable Care Act has got a ton of money out there for community health workers and things like that. But what they will not be able to offer, that this concept does offer, is that when Mrs. Jones leaves the hospital the reason people in the church are going to be willing to do what we need to keep her healthy is they know Mrs. Jones, they care about Mrs. Jones and, the thing you cannot buy, they love Mrs. Jones.”
Endnote: *Tennessee's Republican Gov. Bill Haslam has not decided whether to accept the Affordable Care Act’s federal Medicaid expansion, a program that provides states with several years of federal funding to broaden Medicaid availability. Under the expansion the federal government would cover 100 percent of the difference for a few years after which its share would decline slightly. Republican governors in Arizona and elsewhere have defied GOP orthodoxy to accept the Obamacare money but Haslam remains undecided. Tennessee has about 1 million uninsured people. According to one study, the Medicaid expansion is the difference between insuring one-third of them and more than half of them under Obamacare. If Haslam rejects the Medicaid expansion plan it would be walking away from $22.3 billion in federal Medicaid money through 2022. This would be an audacious move for a governor who has at least tacitly admitted that his state’s poor health is a drag on its economy.
Alex Halperin is news editor at Salon. You can follow him on Twitter @alexhalperin. More Alex Halperin.