Fracture risk 40 percent higher risk if low Vitamin D
Low Vitamin D Status Is Associated With Impaired Bone Quality and Increased Risk of Fracture-Related Hospitalization in Older Australian Women.
J Bone Miner Res. 2019 Jun 24. doi: 10.1002/jbmr.3818
Zhu K1,2, Lewis JR2,3,4, Sim M2,3, Prince RL1,2.
1 Department of Endocrinology and Diabetes, Sir Charles Gairdner Hospital, Perth, WA, Australia.
2 Medical School, University of Western Australia, Perth, WA, Australia.
3 School of Medical and Health Sciences, Edith Cowan University, Joondalup, WA, Australia.
4 Centre for Kidney Research, Children's Hospital at Westmead, School of Public Health, Sydney Medical School,
The University of Sydney, Sydney, NSW, Australia.
📄 Download the PDF from sci-hub via Vitamin D Life
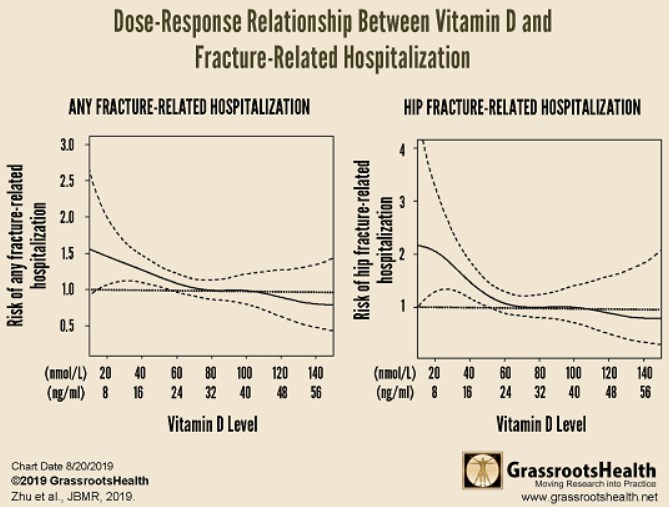
Charts of the data from Grassroots Health

The vitamin D debate relates in part to ideal public health population levels of circulating 25-hydroxyvitamin D (25OHD) to maintain bone structure and reduce fracture. In a secondary analysis of 1348 women aged 70 to 85 years at baseline (1998) from the Perth Longitudinal Study of Aging in Women (a 5-year calcium supplementation trial followed by two 5-year extensions), we examined the dose-response relations of baseline plasma 25OHD with hip DXA BMD at year 1, lumbar spine BMD, and trabecular bone score (TBS) at year 5, and fracture-related hospitalizations over 14.5 years obtained by health record linkage. Mean baseline plasma 25OHD was 66.9 ± 28.2 nmol/L and 28.5%, 36.4%, and 35.1% of women had levels <50, 50 to 74.9, and ≥75 nmol/L, respectively. Generalized additive models showed that total hip and femoral neck BMD and TBS, but not spine BMD, were higher with increasing plasma 25OHD up to 100 nmol/L. Compared with those with 25OHD <50 nmol/L, women with 25OHD ≥75 nmol/L had significantly higher total hip and femoral neck BMD at year 1 (3.3% to 3.9%) and TBS at year 5 (2.0%), all P < 0.05.
During the follow-up, 27.6% of women experienced any fracture-related hospitalization and 10.6% hip fracture-related hospitalization. Penalized spline regression models showed a decrease in risk with increased 25OHD levels up to 65 nmol/L and 75 nmol/L for hip fracture and any fracture-related hospitalization, respectively.
Cox regression grouped analyses showed that compared with women with 25OHD <50 nmol/L, those with 25OHD levels 50 to 74.9 and ≥75 nmol/L had significantly lower risk for hip fracture [ HR 0.60 (95% CI, 0.40 to 0.91) and 0.61 (95% CI, 0.40 to 0.92), respectively], and any fracture-related hospitalization [HR 0.77 (95% CI, 0.59 to 0.99) and 0.70 (95% CI, 0.54 to 0.91), respectively]. In older white women, 25OHD levels >50 nmol/L are a minimum public health target and 25OHD levels beyond 75 nmol/L may not have additional benefit to reduce fracture risk.